
Grantmakers In Health (GIH) is pleased to publish this supplement to Stanford Social Innovation Review on innovations in health equity, and we thank the Aetna Foundation for sponsoring it. GIH is a philanthropic affinity organization that informs and advises health foundations, corporate giving programs, and other funders, and provides opportunities for them to share knowledge and experiences. We are a voice for health philanthropy, and through our programming we advance the field.
Innovations in Health Equity
This special supplement examines the organizations and programs that are addressing social inequalities in housing, transportation, work, and other parts of society that create disparate health outcomes.
-
Innovations in Health Equity and Health Philanthropy
-
Illuminating the Health Equity Challenge
-
Partnering with Philanthropy in Native America
-
Building Power, Building Health
-
Philanthropy on the Frontlines of Ferguson
-
Promoting Health Impact Assessments
-
Building a Healthier Nail Salon Industry
-
Embracing Healing Justice in California
-
Ending LGBT Health Inequities
-
Achieving Healthy Communities Through Transit Equity
-
Using Fair Housing to Achieve Health Equity
-
Reducing Health Disparities in Atlanta
Health equity is an area of intense focus for philanthropy, fueled by a sense of urgency about the need to reverse long-standing destructive trends. It is an area in which health philanthropy has shown consistent leadership in support of innovative work. Our goal in this supplement is to lift up new voices and approaches in health equity and to highlight the work of funders and community organizations that use health equity as a lens for grantmaking and partnerships. Although it was impossible to include profiles of all the good work occurring in communities across the country, we did our best to select a cross-section of programs that are concerned with some of this nation’s most vulnerable populations, such as youth, LGBT people, low-income communities, immigrants, and people of color.
The leading edge of health equity work illustrated here encompasses a wide range of strategies. Settings include LGBT community centers, racially and ethnically diverse urban communities, and rural Indian country. Frameworks include promoting health equity through organizing and advocacy, grantmaking, research and data collection, regional and cross-sectoral collaboration, and community engagement. Many aspire to change policy in order to achieve sustained systems-level change. Consistently, there is a focus on community involvement, which is very different from the perspective of the traditional health-care system.
The work spotlighted in this supplement is energetic and exciting. Progress made from these various strategies will inform our understanding of what works while also—ideally—moving us closer to the goal of improved health for all.
The Quest for Health Equity
The quest for health equity has its roots in more than a century of data showing that morbidity and mortality rates for poor Americans and people of color are significantly worse than those for the white mainstream. Even in the 19th century, the lack of health equity in the United States was a subject of concern for advocates, scholars, and health professionals. For example, in 1899 sociologist W. E. B. DuBois noted in his book The Philadelphia Negro that “[there] is a much higher death rate at present among Negroes than among whites: this is one measure of the difference in their social advancement.”
In 1914, Booker T. Washington commented publicly on the high rate of preventable death among blacks, and in 1915 he organized National Negro Health Week, hoping to generate broad support for improving black health. Black public health leaders sustained this effort by continuing to promote National Negro Health Week for several more decades. In the meantime, trends in black and white health changed little, with large differences between the two groups in life expectancy, chronic disease prevalence, and causes of death.
In 1985, the federal government accomplished Booker T. Washington’s then-70-year-old goal of bringing racial health disparities to national attention with the publication of the landmark Heckler Report, or “Report of the Secretary’s Task Force on Black and Minority Health.” The report’s finding—“a sad and significant fact [is the] continuing disparity in the burden of death and illness experienced by Blacks and other minority Americans as compared with our nation’s population as a whole”—began to galvanize action.
Since 1985, the United States has made some progress in reducing health disparities, but it is far from enough. In fact, the federal Agency for Healthcare Research and Quality’s most recent “National Healthcare Disparities Report, 2014” rated national progress in reducing disparities in health care as “poor.” It concluded that people of color and people in poverty had worsening quality and access on many disparity measures, and that there had been no significant change over time. In addition, the report found that whereas disparities are decreasing in a few areas, such as the number of deaths from HIV, they are continuing to increase in others, such as cancer screening and maternal and child health. The Affordable Care Act (ACA) promises to expand the number of Americans eligible for these and other preventive health services, but it is not a given that health disparities will decrease as a result.
Health Equity and the Social Determinants of Health
Research has consistently shown that race and socioeconomic status are important causes of health disparities. Simply put, disadvantaged social groups systematically experience worse health or greater health risks than more advantaged social groups. From birth to death, race and class have an effect on rates of disease risk, exposure to environmental hazards and socioeconomic stressors, and access to health necessities such as healthy food and safe housing.
The concept of the social determinants of health, introduced by the World Health Organization (WHO) about a decade ago, has been an important tool for explaining how the social and economic structures that shape how people live also affect their health. WHO’s determinants cover a broad spectrum of social, economic, and environmental factors. Included among them are access to health care and education; the distribution of power, income, and goods and services in a community; and other conditions at work, at home, in neighborhoods, and in the surrounding environment.
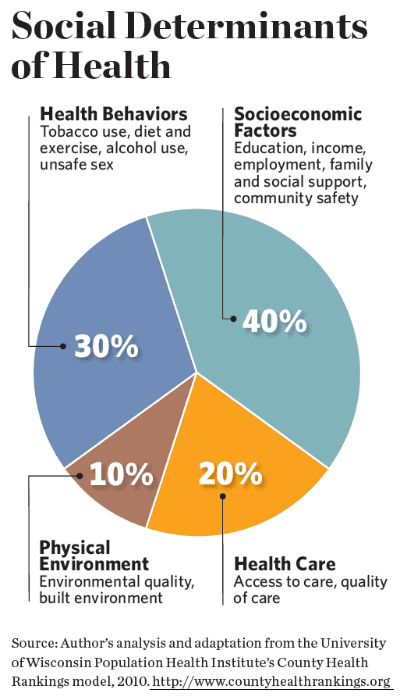
Access to high-quality health services is just one of several contributors to good health status. Once thought to be the key to good health, access is now understood to have about half the influence of education, employment, and other socioeconomic factors. (See “Social Determinants of Health” below.)
Health funders’ adoption of the social determinants approach has required them to think differently about how they want to target their grantmaking in order to support healthy people and communities. The transition has occurred gradually. In the past, many philanthropic efforts to reduce health inequalities focused on individuals. There was an emphasis on primary prevention (such as community health education and screening), improvements in the delivery of health care, and use of data to track trends and outcomes.
With growing evidence of the social determinants of health, health funders began to focus their attention on “upstream” strategies—for example, improving housing or increasing access to education—alongside continued “downstream” work to improve health-care services. Interest in issues like access to healthy food, toxic exposure and other environmental issues, early childhood education, and investing in communities has grown.
Making Progress on Health Equity
Health philanthropy offers several promising examples of progress in achieving health equity. Admittedly, the problem is enormous, and even successful investments can bring about only incremental improvements. Nonetheless, these bright spots lay the groundwork for positive change.
For some funders, supporting equity means working to influence federal policy change. Many did so in the years leading up to the passage of the ACA. Their grantmaking elevated health reform as a critical issue and helped keep it on national and state policy agendas over the course of many years. They also invested in outreach and enrollment activities—especially in low-income communities—and provided sustained support to advocacy organizations and coalitions.
Post-ACA, many health funders continue to support health system reform as one strategy for eliminating health disparities. For example, the Con Alma Health Foundation is partnering with a national funder, the W. K. Kellogg Foundation, to monitor the implementation of the ACA in New Mexico, with a special focus on low-income and rural communities of color.
Other funders are taking a broader view that addresses inequalities by moving beyond health care and, in some cases, outside the health sector. For example, the California Endowment’s $1 billion, 10-year Building Healthy Communities initiative supports health equity, but it intentionally does not fund direct health-care services. Instead, its goal is to “change rules at the local and state levels so that everyone is valued and has access to the resources and opportunities essential for health: affordable housing and fresh food, jobs that are safe and pay fair wages, clean air, and the other ingredients essential for a healthy life.”
Health funders who have partnered with non-health organizations are an example of a growing interest in working across sectors to improve health equity. Many health funders recognize that in low-income urban neighborhoods, community development offers a vital pathway for improving the underlying conditions that shape health. By partnering with community development organizations, they have begun to invest in affordable housing, community clinics, grocery stores, child care, and other health-promoting initiatives.
One example of these partnerships is the Healthy Futures Fund, an initiative of the Local Initiatives Support Corporation, Morgan Stanley, and the Kresge Foundation. The fund supports development of federally qualified health centers in underserved areas, as well as affordable housing that incorporates health programs for low-income residents. If successful, these grantmaking strategies could potentially lead to larger wins and could be an opportunity for health philanthropy to broaden its sphere of influence outside the boundaries of the traditional health sector.
The Road Ahead
Because health equity is ultimately part of the larger issue of social and economic inequality, worsening economic inequality in the United States threatens health philanthropy’s ability to make meaningful improvements. In recent months, the Ford Foundation’s strategic shift to fighting inequality has raised the question of the role philanthropy can play in this arena.
Looking ahead, it is likely that there will be increasing pressure for funders to recognize the structural underpinnings of many social problems—including health disparities—and to commit to transforming those structural elements. This level of effort would require focusing on root causes—in the case of the Ford Foundation, these include the distribution of wealth, education and opportunities for young people, and justice based on race, ethnicity, and gender—and the willingness to take risks, invest for the long term, and work across sectors. Such work would be difficult and controversial, but because of its ability to act independently and break new ground, philanthropy may be particularly suited for taking it on.
Support SSIR’s coverage of cross-sector solutions to global challenges.
Help us further the reach of innovative ideas. Donate today.
Read more stories by Faith Mitchell.