

 Technicians run Swaasa tests at medical units in health camps managed by Child Survival India in Khandala, Maharashtra. (Photo Courtesy of Swaasa)
Technicians run Swaasa tests at medical units in health camps managed by Child Survival India in Khandala, Maharashtra. (Photo Courtesy of Swaasa)
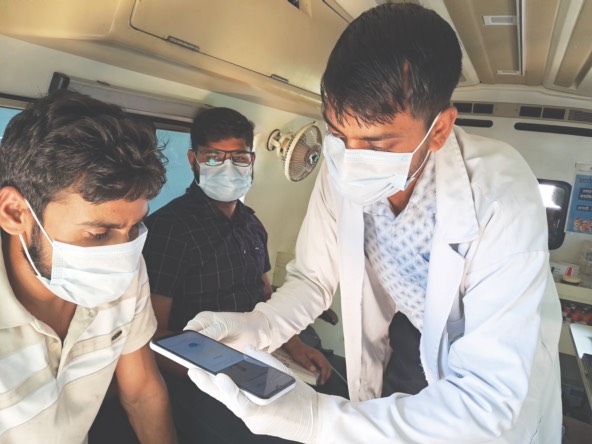
As patients line up outside a mobile medical van parked in a village square in Rajasthan’s rural Behror region, pharmacist Pankaj Kumar Kakodia sanitizes his mobile phone, adjusts his surgical mask, and pulls on disposable gloves. He calls the first patient in, seats her on the bench, and hands her a mask. Opening an app called Swaasa on his phone, he asks the patient a few questions about her symptoms and enters her answers. He then holds the phone up, presses a button to record, and instructs her: “Please cough three to four times in 10 seconds.”
Within minutes, the app indicates whether the patient may be at risk for any respiratory illness. The doctor in the medical van run by the nonprofit Child Survival India reviews the report and prescribes further diagnostic tests.
“If a patient is flagged as high-risk for tuberculosis (TB), we refer them for a sputum test and chest scan at the district hospital,” Kakodia says. “If confirmed positive, they are connected to the government’s TB elimination program for treatment as per protocol. If the screening indicates asthma, bronchitis, or a respiratory infection, our doctors prescribe the appropriate medication.”
India bears the highest burden of TB globally, accounting for 27 percent of all cases and nearly a third of chronic respiratory diseases. Each year, 2.5 million people are diagnosed with TB, and millions more go undetected in India. Despite ambitious targets to eliminate the disease by 2025, a critical gap remains: early, affordable respiratory screening and diagnosis.
Narayana Rao Sripada, founder and chief technology officer of the Hyderabad-based Salcit Technologies, developed Swaasa to bridge this wide gap. Rolled out in 2023, the pioneering AI-powered tool is gradually being adopted for screenings at hospitals, primary health centers, telehealth facilities, and nonprofits running health programs.
Acoustic Signal Analysis
Swaasa’s origins date back to 2015, when Sripada, who then worked in the tech industry, served as an external advisor to academic institutions working on a government project to develop a scalable and affordable health-care solution.
“What began as a virtual assistant was narrowed down to an acoustic signal analysis for health care,” he says. Around this time, Sripada came across global research on the diagnostic potential of acoustics, including studies showing that sounds from the heart, lungs, and coughs carry valuable information.
“Research from Queensland University, for example, had used cough as a marker to detect pneumonia,” he says. “So, we began gathering cough data from medical colleges in India, and our early analysis suggested that cough indeed carries some signatures for various conditions.”
A chance meeting in 2017 with Anand Krishnan, a professor of community medicine at the All India Institute of Medical Sciences (AIIMS), made him aware of a serious unmet need in India’s screening for respiratory diseases, particularly in rural areas. Spirometry is difficult to deploy due to expensive hardware and the need for skilled technicians.
“Over 50 percent of patients who visit these centers have some kind of respiratory issue,” Sripada says. “Dr. Krishnan recommended developing a simple technology that could be used easily by frontline health workers, be noninvasive, and still detect moderate to severe risk for respiratory conditions.”
 Technicians run Swaasa tests at medical units in health camps managed by Child Survival India in Behror, Rajasthan. (Photo Courtesy of Swaasa)
Technicians run Swaasa tests at medical units in health camps managed by Child Survival India in Behror, Rajasthan. (Photo Courtesy of Swaasa)
That insight led Sripada to work closely with pulmonologists to build the first prototype of Swaasa in 2018. His company, Salcit Technologies, received government grants worth INR 40 million ($455,148) from India’s Ministry of Electronics and Information Technology and from the Department of Biotechnology, along with financial support from the US Agency for International Development and the UK Foreign, Commonwealth & Development Office to work on the technology.
Several clinical tests, conducted in collaboration with leading medical research centers in India and abroad, assessed how the app could distinguish normal from abnormal respiratory sounds and identify obstructive and restrictive conditions. Diagnostic tools are measured for accuracy, sensitivity (effectiveness at detecting a positive case of disease), and specificity (effectiveness at identifying a negative case—i.e., a person who does not have a disease).
“For detecting normal versus abnormal sounds, our accuracy is about 90 percent, with 92 percent sensitivity and around 85 percent specificity,” says Sripada, who has also secured patents for the product. “For obstructive conditions, accuracy is about 85 percent, with 80 percent sensitivity and 75 percent specificity. And when it comes to narrowing down specifically to pulmonary tuberculosis, our sensitivity is around 80 percent, with specificity at about 65 percent.”
Once Swaasa had scientific validation and use cases, scaling it required a stronger team and infrastructure. In May 2020, Manmohan Jain and Venkat Yechuri formally joined from Zensark Technologies as cofounders—Jain to lead operations and Yechuri as chief executive officer. Zensark also invested about $1.2 million to help scale the product. During the COVID-19 pandemic, Swaasa was repurposed for screening by a few private health-care operators as well.
By 2023, Swaasa had regulatory approval and officially launched with financial support from the India Health Fund and ACT for Health. “We believe that actively finding undiagnosed TB cases quickly and connecting them to treatment will bring us closer to the elimination of the disease,” said Madhav Joshi, CEO of the India Health Fund, in a press release.
Swaasa has so far screened more than 400,000 people, predominantly in semi-urban and rural areas, with studies showing 50-60 percent cost savings and 40-50 percent faster turnaround compared with traditional methods of screening. With subscription-based and pay-per-use pricing models that keep test costs between INR 100 and 350 ($1.20-$4.20), depending on level of risk detection and analysis, it is currently in use across health centers in Delhi, Bihar, Uttar Pradesh, Odisha, Andhra Pradesh, Telangana, and Karnataka. Salcit also claims to have the world’s largest annotated cough database across seven countries and is collaborating on research with the University of California, San Francisco; the University of California, Irvine; and St. Francis Xavier University in Canada. In 2024, Salcit also partnered with Google to expand its AI model to improve accuracy and scalability.
Driving Referrals
Swaasa’s growing success depends on its wide applicability and flexibility on the ground. “We have partnered with a number of organizations—pharma companies, hospitals, nonprofits, wellness centers, insurance, research and development, corporates, housing units,” says Nyamat Bindra, who leads deployments and operations in North India. “We also regularly train field-workers, community health workers, and doctors on how to use the app. The model is agile, and available in multiple languages so it makes adoption easier.”
Doctors report that the app can be particularly useful in community settings where advanced diagnostics are not readily available.
The key, she adds, is driving referrals, ensuring follow-ups, and helping break stigma around TB. “If we see more prevalence of certain respiratory conditions in a certain vulnerable community, for example, we increase the number of screenings there,” she says. “Even in difficult terrains and low-resource settings, Swaasa can be used without the internet. We always tell patients we are not replacing doctors, but aiding them.”
Swaasa has high acceptability among patients, organizations have found, because it is a simple, low-cost tool built into smartphones and noninvasive. “It has been useful to screen patients early, so that potential cases don’t go undetected and spread within families,” says Deepa Bajaj, chief executive officer at Child Survival India, a nonprofit that supports health programs for vulnerable communities such as migrant laborers, construction workers, and truckers.
“We have done screenings using the Swaasa app for over 14 months, including for truck drivers in Maharashtra, since they are exposed to fumes and pollution and are therefore vulnerable to respiratory illnesses, and in villages across Rajasthan through our mobile medical vans,” Bajaj says. “It is often difficult to convince patients to undergo chest scans, even when they show symptoms. But when the Swaasa app identifies them as ‘high risk’ for TB, it is easier to counsel and refer them for confirmatory tests and link them with the government system to ensure proper treatment and monitoring.”
Doctors who have used the tool to screen patients report that the app can be particularly useful in outpatient settings where medical professionals are often pressed for time, or in community settings where advanced diagnostics are not readily available. “We found the tool to be reasonably sensitive—around 75-80 percent during our study of over 6,000 patients across multiple sites in India,” says Rakesh Kumar, MBBS, MD, an epidemiologist and additional professor at the Centre for Community Medicine at AIIMS. “The most important factor holding India back from eliminating TB is a diagnostic gap. A technology like Swaasa offers utility and works well to identify patients who need further testing.”
One such patient is 22-year-old Siraj Singh (name changed to protect his identity), a mechanic based in Faridabad, a suburb of New Delhi. “I had a persistent cough for weeks, which didn’t go away despite consulting a private doctor,” he says. So, he went to a Swaasa screening camp near his home last December and discovered that he was at high risk for TB. Doctors advised him to distance himself from his family and referred him to a government hospital, where he had his diagnosis confirmed, received treatment, and fully recovered. “Thankfully, my family was safe from the disease because we knew the precautions to take once I was diagnosed,” he says.
With the growing adoption of AI in health care, a few other organizations in India are also experimenting with cough-based models to detect respiratory conditions. But Swaasa holds an early-mover advantage as the first to secure regulatory approval and a wide cough database. The current focus, says the team, is on deeper integration into India’s health ecosystem, across public and private health care.
“Even when used in hospitals as a screening tool, the primary challenge is embedding it into routine testing, as it is a completely disruptive innovation,” Sripada says. Salcit is now working on a number of new partnerships with state governments in a race to widen its reach—and prevent more TB cases from slipping through the cracks.
Read more stories by Neha Bhatt.