

 (Illustration by Jon Krause)
(Illustration by Jon Krause)
It’s no secret that our health, education, and social service systems are failing the people they intend to serve. The US infant mortality rate is higher than in most developed countries, and the gap is widening. American children’s educational performance ranks very low in comparison with the 35 other Organisation for Economic Co-operation and Development (OECD) countries. The United States incarcerates people at a rate far higher than that of any other nation, and prisons have become the de facto mental health system for many people diagnosed with serious mental illness. Intergenerational poverty and violence are persistent, particularly among groups that have faced historical discrimination. More recently, the opioid epidemic has presented complex social challenges that are extremely difficult to unpack and address.
While a majority of participants in social and educational programs make progress, some flounder. Over time, this pattern has reinforced the mistaken belief that social problems are inherent in individuals, rather than created and sustained by environmental conditions.
The science of trauma has opened new pathways for understanding and addressing social problems resistant to traditional programs and services. Beginning with the seminal Adverse Childhood Experiences (ACE) study, which the US Centers for Disease Control and Prevention published in 1998, a growing body of research has demonstrated that adverse experiences and chronic stress, particularly in childhood, can harm the developing brain. Repeated exposure to perceived danger alters the connections between brain cells and floods the body with hormones. These biological changes accumulate over time and can have long-term consequences for emotional function, regulatory capacities, physical health, and successful performance in a variety of domains, such as education, parenting, and employment. Research in the field of epigenetics has even suggested the possible biological transmission of trauma from generation to generation.
A mix of genetic and environmental influences determines physical and mental health. This combination of factors helps to explain why individuals or groups that are exposed to the same trauma may experience different outcomes. Treatments, environments, and cultures that do not recognize the biological impact of repeated trauma may be ineffective or even cause additional harm by retraumatizing those they serve. Behavioral health organizations are increasingly providing evidence-based, trauma-specific therapies. However, therapy alone does not eliminate the risk of an organization’s activating a trauma response, nor does it address the wide range of consequences of traumatic exposure. Trauma-informed organizational models are necessary to address these more systemic issues.
The changes that an organization needs to make to become trauma-informed are difficult to pinpoint and even harder to sustain. A developmental model of trauma-informed organizational change, such as the Missouri Model, can make the process seem less daunting by providing options and a road map for the journey. By breaking down the process and identifying primary indicators of change, a trauma-informed developmental approach can help guide organizations and communities toward the deeper, systemic change required to address seemingly intractable social problems.
Trauma Science
Trauma science intersects with the body of research on resilience, generally defined as the ability to recover from or adjust easily to misfortune or change. In the parlance of prevention, traumatic experiences are risk factors for a variety of negative outcomes, while “resilience” refers to internal strengths and external supports that buffer the impact of adversity. One of the most consistent findings in decades of prevention research is that environmental supports, or protective factors, such as caring relationships, high expectations, and opportunities for meaningful participation, can moderate the impact of trauma, and adversity more generally. The majority of children and youth, even those from economically or socially stressed families or underserved communities, overcome these risk factors and achieve good developmental outcomes.1 In an attempt to integrate these two perspectives, many health and human-service practitioners strike a balance between acknowledging the negative impact of traumatic experiences and recognizing the positive human capacity for resilience and growth. The first provides motivation for developing preventive interventions and new forms of practice, while the latter offers hope to youth, families, caregivers, and providers.
This new trauma and resilience lens has led to the recognition that services may be failing in part because social problems have been incorrectly diagnosed. An incorrect diagnosis often leads to ineffective and even counterproductive interventions. Once researchers have identified underlying causes, new solutions arise naturally. For example, epidemiologist Gary Slutkin has shown that conceptualizing violent behavior as the result of previous experiences of violence, rather than as a personal failing, reframes violence as a public health epidemic.
Societal awareness of, as well as scientific knowledge about, traumatic events has increased dramatically since the 1998 ACE study. Prior public attention had focused largely on post-traumatic stress disorder (PTSD) in veterans returning from military action2 and, to a lesser extent, on the effects of child abuse and violence against women. The ACE study directed both professional and public attention to the impact of 10 family-related adverse events occurring in childhood.3 Since then, the psychological harm caused by a wide variety of events and circumstances, including disasters, social violence, racism, and poverty, has received increasing attention.
As recognition of these events and circumstances has grown, so too has the need to discriminate between experiences that can have a lasting psychological impact and those that are merely stressful. While no single accepted definition of psychological trauma exists, a growing number of organizations use the definition that the federal Substance Abuse and Mental Health Services Administration (SAMHSA) has developed:
(Psychological) trauma results from an event, series of events, or set of circumstances experienced by an individual as physically or emotionally harmful or life threatening that has lasting adverse effects on functioning and on mental, physical, social, emotional, or spiritual well-being.
This definition focuses on how people’s unique experiences can lead to changes in their ability to function, and is consistent with research showing that the biological effects of traumatic events are similar regardless of the source of trauma, and that the more traumatic the events or circumstances, the more severe the consequences to health and well-being.
The American Psychological Association first recognized PTSD as a diagnosable condition in 1980, and early trauma-based therapies focused almost exclusively on treating the symptoms of PTSD. In the 1990s, SAMHSA funded a five-year study of treatment interventions for women with co-occurring mental health and substance use disorders and histories of violence. In the following years, clinicians developed a wide range of treatment models—many of which have been carefully evaluated—to address the consequences of chronic and complex traumatic exposure. Although helpful for individuals in therapy, these models do not address the fact that people with a history of trauma are also involved with various organizations with missions other than mental health. Unless organizations understand the consequences of trauma and know how to respond, they will not be effective in assisting individuals with a significant trauma history. Agencies and services designed to help may instead do significant harm by activating trauma responses, such as self-injurious behavior, aggression, and academic disengagement, and by potentially contributing to cycles of violence and poverty, the overuse of psychotropic medications, or self-destructive behaviors like self-medicating with recreational drugs. Institutions like schools, churches, health and human services, and the military may inflict harm on people who depend on them for safety and well-being. Psychologists Carly Smith and Jennifer Freyd have called this process “institutional betrayal.” 4
The term “trauma-informed” was first used by clinical psychologists Maxine Harris and Roger Fallot to describe the organizational context necessary to respond effectively to violence and trauma in the lives of people with mental health problems.5 Over the next decade, the concept was applied across multiple service sectors. Unlike trauma-based treatments, trauma-informed models involve changing the culture and operating norms of an entire organization or setting. According to SAMHSA:
A program, organization, or system is trauma-informed when it realizes the widespread impact of trauma and understands potential paths for recovery; recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system; responds by fully integrating knowledge about trauma into policies, procedures, and practices; and seeks to actively resist re-traumatization.
Growing evidence suggests that trauma-informed organizations—those that have policies, practices, and environments reflecting the science of trauma and resilience—can reduce long-term consequences of trauma for individuals and society. We now hear about trauma-informed classrooms, health-care clinics, mental health and addiction services, juvenile justice and child welfare programs, courts and law enforcement, jails and prisons, faith communities, and workplaces. Several states have adopted a trauma-informed framework for their entire human service system, and a number of districts and municipalities have embraced the goal of becoming trauma-informed communities. This uptake is not altogether surprising, since trauma-informed models share two characteristics that promote social diffusion: They have the potential to make providers’ work easier, and they address visible and immediate problems.6
“Incomplete implementation may be as bad as—or worse than—the status quo, since institutional betrayal can exacerbate trauma symptoms.”
New Solutions Through a Trauma Lens
While few comprehensive evaluations of trauma-informed organizational change efforts have occurred, studies demonstrate that introducing trauma-informed practices can lead to greater client and family satisfaction, positive client outcomes, increased hope and optimism, and decreased trauma symptomology. Perhaps the best-known example of trauma-informed change is documented in Paper Tigers. The film features Lincoln High School, an alternative school in Walla Walla, Washington, for youth who are failing in regular public schools, many of whom come from disadvantaged backgrounds. The level of childhood trauma among students at Lincoln High (measured by baseline ACE scores) was four times the statewide average. Starting in 2009, the school’s principal Jim Sporleder spearheaded an effort to encourage the school’s support of traumatized youth, build youth resilience, and increase student capacity to learn. The initiative focused on reinforcing trauma-based values and behaviors among teachers and staff; between teachers, staff, and students; and among students themselves. Within a few years, discipline problems and suspensions had decreased and the student retention rate had increased. In 2013-2014, researchers conducted a study to measure student resilience and its relationship to school performance. Results showed that resilience had increased significantly; increases in resilience were related to school performance (both grades and standardized test scores), and resilience moderated the expected negative effects of childhood trauma.
A second example of trauma-informed change that has received national recognition occurred on the Menominee reservation in Wisconsin. The initiative began in 2009, when tribal officials began to understand that poor academic performance by and health problems of tribal youth were related—and that both were tied to trauma. The officials initiated a process of engaging and educating the tribe about the effects of a century of historical trauma, while simultaneously integrating trauma-based practices in health care, education, and social services.
Menominee leaders understood that many ongoing sources of trauma, including high rates of intimate-partner violence, substance use, and child maltreatment, could be seen as manifestations of a loss of tribal identity and culture. This pervasive historical trauma stemmed from government policies beginning in 1860 that required children under the age of 15 to go to boarding schools where tribal language and customs were banned. Forced assimilation continued between 1954 and 1973, when Congress terminated the Menominees’ legal identity and rights. These policies not only traumatized the tribe but also weakened the traditional family and social structures that normally serve as protective factors. Governmental programs that offered culturally unsuitable “standard” models of health care and social services continued this pattern. As intergenerational trauma became widespread and natural protective factors fell off, maladaptive coping became the norm.
With this understanding, the Menominee tribe framed trauma as a community—rather than an individual or family—problem and made sure that traditional cultural practices played a key role in trauma-informed interventions. For example, Menominee culture views pregnancy as a sacred state of life and considers keeping women and babies safe and healthy an honorable form of living. The tribe now affirms these values by teaching high school students the Menominee Grandfather Teachings (wisdom, love, respect, bravery, honesty, humility, and truth), and providing girls with culturally relevant reproductive health and support services. Similarly, the Menominee tribe has established drug-free cultural events, such as an annual sobriety powwow. Between 2008 and 2013, annual births among girls ages 15 to 17 dropped from a high of 20 births to fewer than 5; rates of substance use among high school students declined, including use of marijuana (30 percent decrease), cigarettes (49 percent decrease), and alcohol (64 percent decrease); and high school graduation rates increased from 60 to almost 99 percent.7
Case studies like these demonstrate that solutions that incorporate a trauma-informed framework can improve outcomes. However, significant barriers to their effective use as a strategy for systems change remain. While many leaders in the field emphasize the importance of integrated, systemic change, psychologist Kathryn Becker-Blease has pointed out that in practice, the term “trauma-informed” is often used to describe a variety of discrete services delivered in isolation.8 Change efforts often focus on individual healing, rather than on broader organizational or policy reform. An agency may describe itself as trauma-informed when in fact all it has done is added a new trauma clinician or treatment option to its service menu or begun offering basic training to staff. The lack of clarity about what constitutes “trauma-informed change” impedes communication, implementation, and evaluation. As a result, trauma survivors who anticipate more respectful treatment, and advocates who anticipate structural reform, might be disappointed.
Incomplete or ineffective implementation of trauma-informed approaches may be as bad as—or worse than—the status quo, since institutional betrayal can exacerbate the symptoms of preexisting trauma. For example, sexual assault survivors whose experiences are minimized or covered up by the institutions to which they report the assault later experience higher levels of trauma symptoms.9 Moreover, trauma-informed organizational or community change is not yet the norm in any field, perhaps in part because of the complexity of the implementation process. Many organizations are likely to perceive a culture change of this magnitude as too time-consuming and resource-intensive. Even in organizations that make a significant commitment to becoming trauma-informed, like the San Francisco Public Health Department,the change process may stall when initial enthusiasm wanes or when expectations about the speed with which change will occur are not met.10
“A developmental process-based approach to trauma-informed change holds the potential to guide us toward deeper systems change.”
The Missouri Model
Like most other models of trauma-informed organizational change, the Missouri Model is based on a set of principles (safety, trustworthiness, choice, collaboration, and empowerment) that reflect an understanding of the effect of trauma and provide a new template for practice. It is also similar to several other models in providing a tool for conducting an organizational self-assessment.11 However, unlike other systems, the Missouri Model explicitly conceptualizes being “trauma-informed” as the end result of a developmental process in which the organization goes through a series of successive stages.
The model grew out of a three-year trauma-informed “early adopters” initiative that Patsy Carter (this article’s coauthor) oversaw while working with the Missouri Department of Mental Health (MODMH). Five community mental health centers, a state-operated children’s residential center, and the state office of the Division of Youth Services participated in this project. They received intensive training and ongoing consultation and participated in annual summits to share experiences. At the end of three years, MODMH convened a statewide “trauma roundtable” that included the early adopters and other organizations in the state that had shown leadership in addressing trauma. Members reflected different professional roles (including, but not limited to, research, disaster response, and evidence-based clinical practices) and a variety of different service systems (including domestic violence, juvenile justice, child welfare, substance use, and mental health). The purpose of the roundtable was to identify needs and areas of focus and to develop a statewide change strategy.
The early adopters had already encountered many barriers to effective systems change. They had come to no consensus on language or definitions and had no basis on which to evaluate provider claims of being trauma-informed. These obstacles were particularly troubling when it became clear that training had been superficial or that retraumatizing practices still occurred. The early adopters also noted that many agencies in their communities were intimidated by the scope of change involved, and that not all agencies saw their mission as equally aligned with a trauma-informed framework. The roundtable concluded that an effective implementation system would clearly define terms, establish a developmental framework, emphasize the importance of structural change, provide guidance on measuring progress, and allow organizations to make decisions about how far and fast to go. Over the next two years, the roundtable developed the Missouri Model to meet these goals and encouraged the state to adopt it in all trauma-related efforts.
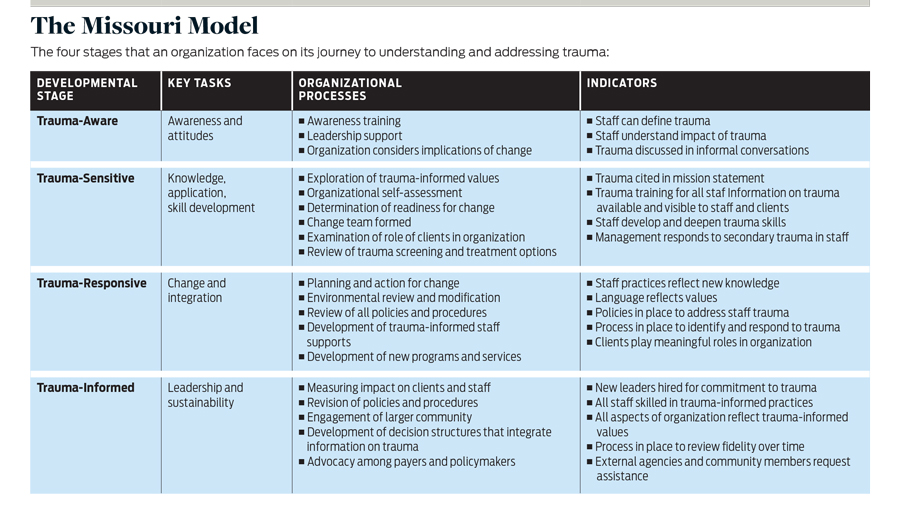
The Missouri Model proposes a continuum of four stages or levels that an organization can attain on its journey to understanding and addressing trauma. At each level, the model identifies major tasks to accomplish, organizational processes likely to be helpful, key indicators that the organization has reached this stage, and links to resources. (See “The Missouri Model” on page 53.) Stages are not uniformly sequential or mutually exclusive—agencies often reflect different developmental stages in different domains and may move back and forth between stages over time. Some agencies may complete specific tasks earlier or later than the model proposes. Nonetheless, many agencies find it helpful to think about a continuum of implementation, rather than seeing the process as a dichotomy of trauma-informed versus uninformed.
The implementation process used by one of the early adopters, Truman Medical Center (TMC) in Kansas City, Missouri, shows how a developmental framework can guide change. Initial steps at TMC focused on trauma awareness, including offering an all-staff introductory training program, hosting an agency-wide open house, and assessing clinical staff’s ability to provide trauma-specific services. As awareness and enthusiasm grew, TMC began working on trauma sensitivity, institutionalizing in-depth training, and paying close attention to how embracing trauma-informed principles would affect current practice. This step helped staff to see that addressing trauma was not just an additional responsibility but a new way of thinking that made their jobs easier and their work environment more supportive. At this point, each department completed a trauma-informed organizational assessment and developed a set of separate goals for addressing support of consumers and staff.
During the next stage, TMC worked to make the agency trauma-responsive by changing both client services and staff training.Client-oriented examples included revising no-show policies to provide more ways to remind clients about their appointments, making reasonable accommodations when people were late or came on the wrong day, and creating modified open access. Staff-oriented action items included increased positive recognition, the development of a peer response system for adverse events, improved debriefing processes, and implementation of trauma-informed supervision training. During this stage, the organization also conducted an environmental review and made significant modifications to create openness, light, and a feeling of spaciousness, as well as improving signage to make the building easier to navigate.
As TMC moved closer to the trauma-informed stage, it began to see measurable changes in outcomes. Programs that had implemented open access saw a decrease in no-show rates. As results improved and costs decreased, TMC began to build a strong business case for trauma-informed organizational change. Relationships between staff and consumers and between supervisors and staff showed a higher level of trust, less judgment, and more understanding as the organization’s knowledge of how toxic stress and trauma affect brain functioning and perceptions increased. Access to evidence-based behavioral health treatments for trauma also improved, as did TMC’s ability to manage more severe mental health symptoms and behaviors. Within a few years, TMC became recognized as a trauma leader in Kansas City, helping to initiate a citywide effort and starting a national Center for Trauma-Informed Innovation. While TMC still has a long way to go, it has already effected positive changes within the population it serves and for its staff.
A second example highlights how a developmental model can guide self-assessment and monitoring. A group of 22 schools in the St. Louis area participated in a trauma-informed learning collaborative (TILC), designed to build leadership among teachers and support staff, led by a local change initiative called Alive and Well STL. The TILC used the Missouri Model to introduce trauma-based practices to teachers and classrooms, starting with three days of intensive training and followed by monthly interactive webinars and quarterly face-to-face meetings. Consultants also conducted site visits to support individual schools in addressing unique challenges.
During the initial stages, the TILC used the Alive and Well Organizational Assessment (AWOA), a tool based on the Missouri Model, to help schools identify areas of focus and establish a mechanism for monitoring progress. Each school’s implementation plan and process were unique. Examples of changes included establishing a trauma committee focused on stress awareness and self-care; honoring community losses; equipping classrooms with sensory tool kits to help children manage emotions; creating a parent group focusing on mindfulness; creating sensory and calm-down rooms for children; implementing mindfulness practices during class periods; and creating a staff calming room for teachers who need to access the space during instructional hours.
Throughout the process, the TILC used multiple evaluation strategies. Overall, participating schools showed an improvement on all seven subscales of the Attitudes Related to Trauma-Informed Care (ARTIC) Scale, a psychometrically validated measure of attitudes toward trauma-informed care.12 Data from several schools also showed a consistent decrease in the number of daily student disciplinary actions. At 6, 12, 18, and 24 months, schools used the AWOA to rate themselves on key indicators for each level of the Missouri Model. At six months, schools rated themselves highest in the “trauma-aware” category, and ratings decreased for the same items at each successive stage. By the end of the project, schools had increased their ratings of items at all four levels. During the last six months, the smallest change (15 percent) was in the area of trauma-aware items and the greatest change (41 percent) was in trauma-informed items, reflecting the shift to the higher-order processes reflective of the trauma-informed stage.
Trauma-Informed Systems Change
A developmental, process-based approach to trauma-informed change highlights the ways in which the work involves fundamental reform of existing support systems for both staff and clients. It immediately draws attention to the dimension of time, emphasizing that trauma-informed change requires a long-term commitment. It highlights the complexity of altering entrenched attitudes, behaviors, and systems, and it makes it clear that change involves a lot more than staff training and new treatment models. It therefore holds the potential to guide us toward deeper forms of systems change.
One process-based, trauma-informed model that presents a developmental trajectory for change has shown significant results at the population level. The Self-Healing Communities Model (SHCM) is based on more than a decade of community-building and culture change in the state of Washington. Population-based health outcomes improved dramatically as communities shifted cultural patterns, gained new knowledge and skills, and began identifying and reflecting on underlying assumptions. The SHCM process consists of four phases: leadership expansion, focus, learning, and results. Much like the Missouri Model, SHCM allows time for reflection and inquiry and emphasizes intentional changes to policies, practices, and day-to-day interactions.
In its home state, the Missouri Model has already helped to facilitate cross-sector collaboration, which is essential in addressing complex social issues. By creating a common language and conceptual framework, the Missouri Model has supported new partnerships among local school systems, community mental health centers, prevention programs, and health-care providers. By bringing together groups and sectors that traditionally work in isolation, it forms the basis for a widespread public health response. At the policy level, the Missouri Model has provided a template for the development of statewide policy guidance on organizational readiness, trauma screening, and trauma-informed human resource practices. A guidance document that translates the Missouri Model into educational language for schools was released in early 2019. The roundtable also developed Missouri’s Comprehensive Public Health Approach for Resilience to Mitigate the Impact of Trauma to assist communities in addressing systemic issues by applying universal strategies to reduce trauma exposure and impact.
Other states have also adopted the Missouri Model. Wisconsin has used it as a statewide planning guide, renaming it the Wisconsin Model and adding Wisconsin-specific resources. Oregon and Delaware have both employed the model statewide, with only minor adaptations. The Ohio Domestic Violence Network, a statewide coalition of domestic violence programs, has used it to create a trauma-informed “road map” for its services, and the state of Illinois is applying it to the public health system. Individual organizations across the country have also treated the model as a template, and Los Angeles County has cited it as a key tool for building trauma-informed communities.
Honest self-reflection is essential to the model if we are to avoid institutional betrayal and retraumatization in services and programs. For example, one of the key principles in most trauma-informed models is empowerment. This principle is particularly important because people so often experience trauma in situations of unequal power, whether interpersonal or institutional. However, implementation of this principle often lags behind others because it directly challenges the power hierarchies present in organizations and communities. Even programs and practices grounded in a philosophy that challenges underlying power dynamics tend over time to slip back into hierarchical formulations and relationships.
Clear definitions and criteria are likely to be increasingly important as the concepts and terminology of trauma-informed models become more common. In 2018, two pieces of federal legislation (addressing foster care placements and the opioid epidemic) tied federal funding directly to trauma-informed approaches. As states face the task of determining what organizations are trauma-informed and therefore eligible for funds, the Missouri Model, or versions thereof, may be essential for developing standards and criteria.
The emerging science of trauma provides new hope for creating more effective service systems and for solving social problems long considered intractable. But to realize the potential of new trauma-informed models, we must clearly define terms and measure impact, as well as unearth, examine, and address the larger social and structural forces that hold currently dysfunctional responses in place. If we do not identify and counter these forces, they will inevitably subvert even the best-intentioned efforts. A developmental, process-oriented approach to trauma-informed change does not guarantee success, but it raises hard questions that we must answer to create service systems and communities that can respond effectively to trauma and violence.
Read more stories by Patsy Carter & Andrea Blanch.