

 (Photo by iStock/PeopleImages)
(Photo by iStock/PeopleImages)
The US has a massive shortage of Black, Latinx, and Indigenous professionals in high-skill health-care roles. Black Americans are only 4 percent of physicians and less than 7 percent of recent medical school graduates—despite making up 13 percent of the population—and the proportion of Black men in medical schools has actually dropped over the past 40 years (the share of Hispanic men and women has stayed constant, while Black women have shown some growth). This lack of diversity fuels gaps in health outcomes: Research shows that patients that share racial identity with their doctors accept more preventative treatments, show better awareness of their medical risks, and adhere more closely over time to doctors’ instructions. One recent study documented a 15 percent reduction in inpatient mortality when Black patients were paired with Black doctors. Another clinical study found a 19 percent reduction in the Black-white mortality gap for outpatient cardiovascular care with patient-physician race-match.
Black, Latinx, and Indigenous communities are not only underrepresented in leadership: They are overrepresented in low-paying support roles. Indeed, there is already a significant talent pool of the Underrepresented in Medicine (or URM); they are simply segregated at the bottom of the career ladder. 59 percent of direct care workers in the United States are BIPOC and 86 percent are women, but they are often underpaid, under-supported, and suffer from high turnover rates (15 percent live below the federal poverty level.) During the pandemic, the vulnerability of health-care support and direct care workers became especially apparent: More than 3,600 US care workers died in 2020, many deemed “essential” yet lacking basic PPE, training, or hazard pay. The majority of direct care and health support workers will not go through baccalaureate programs and lack accessible options for upskilling and career progression.
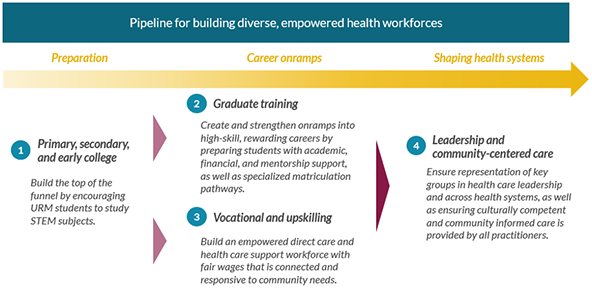
To address these systemic challenges, philanthropic actors must fund all along the pipeline, from children in K-12 all the way to health systems leadership. Each area involves a range of organizations and activities that support URM at different stages of their medical careers, and requires being grounded in local, institutional ecosystems, as well as in the needs of underserved communities:
In California’s Central Valley, for example, UC Davis School of Medicine specifically seeks to address the health needs of local underserved populations by prioritizing future physicians from these communities, where Latinx represent around 70 percent of the population, yet only 5 percent of the physicians, 8 percent of nurses, and 4 percent of pharmacists. In addition, many localities in Central California have half of the physicians recommended for the population size, with rapidly growing demand. To grow the number of enrolling URM medical students, UC Davis must develop a contiguous pipeline that considers the support that local high schools are providing for STEM students, pipeline partnerships with minority-serving community colleges, and specialized enrollment and scholarship programs to ensure these students matriculate. After their graduation, the medical school partners with residency programs to remove barriers for the new physicians to serve in their home communities and address key regional health needs. As a result, UC Davis was ranked this year as the most diverse medical school on the West Coast, with nearly 40 percent of its students joining from URM groups in 2020.
1. Entering the Pipeline
Nearly all experts emphasize the importance of in-school and extracurricular support for primary, secondary, and early college students, for a strong start. If students are not empowered to follow STEM studies at an early age, they are much less likely to pursue higher-level studies. However, minority districts in high-poverty areas receive an estimated $1,200 less per student annually from public sources, leading to inferior facilities, fewer highly experienced teachers, and fewer curricular and extracurricular options. Philanthropic funders have invested hundreds of millions of dollars to ensure children of all socio-economic backgrounds have these resources, but the gap persists.
Philanthropy can play a key role supporting community-based programs to ensure that students can see themselves in medical fields and understand the path to get there. While there is need for more resources across this area, we see two specific opportunities:
- Creating second chance pathways: Many URM students fall out of the system before even making it to medical school applications. These students disproportionately lack support resources and exposure to professionals that come from similar backgrounds to their own. There are three major drop-off points: (1) matriculating from one school to another (e.g., high school to college, community college to four-year institutions, etc.), (2) the first or second year of STEM college courses, and (3) standardized testing. For example, Black males are less likely to retake the MCAT after a low score compared to any other group. Secondary and early college students need support to re-apply, re-train and improve, or to receive informed advice for alternative pathways available, such as health-related associates degrees after high school graduation or post-baccalaureate medical programs after college.
- Bridge programs connecting different educational stages and extending support: Transitionary periods when URM students are moving from minority-serving institutions—such as undergraduate HBCUs, community and tribal colleges, and mentorship programs—into schools outside of their community contexts are significant drop-off points. But programs that bridge high school to college, or community/tribal college to four-year schools, can support students through the changes, as can programs that bridge school to career transition and preparation, such as Health Career Connection.
2. Disrupting the Existing Higher Medical Education System
Philanthropy has recently begun granting long-overdue resources into expanding HBCU programs, which is hugely important. However, to truly scale the number of Black dentists, doctors, and high-skill medical professionals—as well as reach other underrepresented populations such as Latinx and Native Americans—the broader medical education community needs to take a larger role. As Dr. Montgomery Rice of the American Medical Association put it, “We cannot absolve the other 151 medical schools of their responsibility [to help diversify the physician workforce].”
“It’s not just about support, it’s about reorienting education,” as Dr. Michelle Ko, Co-Director of the Center for a Diverse Health Care Workforce at UC Davis put it, “The current medical admissions process does not serve URM students or our communities.” For this reason, select medical schools have begun to prioritize diverse classes of doctors and to focus on the needs of underserved communities. Before 2015, the four HBCU medical schools were graduating more Black doctors than the next 10 schools combined. But the trend has shifted and 2019 was the first year where non-HBCUs graduated more than 90 percent of Black doctors, fueled by public universities such as the medical colleges at Augusta University in Georgia and University of Indiana. The trend holds across other underrepresented groups as well: The top schools graduating Latinx doctors outside of Puerto Rico were University of Illinois, University of Texas, and Florida International University, with public universities also holding the top three slots for Native American doctors. Eight out of the ten most diverse medical schools are public.
Philanthropy can play a catalytic role here. Institutions with successful programs require resources to expand, and other institutions need to be incentivized to follow their lead. Dalberg has identified three high-level opportunities for philanthropic funders to engage:
- Help medical schools to grow their pipeline and provide specialized pathways, both before matriculation and after graduation. To ensure access, graduate medical schools need to build contiguous pipelines into underserved communities to support URM students in their secondary and post-secondary studies. This involves supporting partnerships with minority-serving institutions as well as post-graduate opportunities to practice in their communities. It can also involve special enrollment programs, including BA/MD and post-bac pathways.
- Fund BIPOC faculty chairs and institutional anti-racism efforts. Currently, fewer than 10 percent of full-time medical faculty identify as Hispanic, Black, or Indigenous. The number of faculty chairs held by underrepresented community members is a key factor in determining diverse enrollment. Diversifying faculty positions should be part of larger anti-racism approaches and changes within the institution, such as providing support for URM faculty to pursue research on health equity topics and develop curricula.
- Ensure funding for programs is catalytic and sustainable by requiring matching public funds. Public universities are under tremendous budgetary pressures, especially following COVID-19 cuts to state education funding. This, in turn, increases reliance on tuition funding and away from initiatives targeting low-income students. Philanthropic funding should not try to replace public funding; instead, strategic funders can require matching public funding to help change the incentives faced by university administrators to funnel scarce resources into diversity initiatives.
3. Advancing Support and Direct Care Workers Into Higher-Skill, Better-Paid Roles.
The US health-care workforce is predominantly low-wage support and direct care positions, roles such as home health aides, nursing assistants, and technicians. Health-care support occupations are expected to grow at 4x the rate of all jobs in the economy. Considering the current funnel of workers, that leaves a huge shortfall, especially for roles supporting underserved populations. Making these positions more attractive and providing advancement opportunities is key; however, the ecosystem is complex. The most effective strategies will center on facilitating partnerships in the education-to-employment pipeline.
In line with Dalberg’s previous article on equity in the US care economy and the role of private investment, there is a significant opportunity to build out the infrastructure supporting care providers and those aspiring to enter careers in this space. We firmly believe that a multi-sector, multi-actor response is needed to solve the challenges.
For example, philanthropy can facilitate the ecosystem of employers and community colleges/career training centers. The majority of workers in this space will not go through baccalaureate programs; community colleges are the largest trainers of the health workforce in the US, with health professions ranking as the third most popular category of associate degree nationally. Associate degrees in nursing (ADN) programs educate more than half of all minority nurses and are a key first step towards ascending the career ladder to high-paying registered nurse (RN) positions. There is a significant need to provide upskilling and career entry pathways that fit the needs of mid-career adult learners from underserved communities. For example, over 40 percent of California’s community college students are older than 25 and already working, 69 percent are BIPOC, and the system awards around 6,400 nursing degrees per year. A common career ladder, home health aide (HHA) to certified nursing assistant (CNA) to licensed practical nurse (LPN) to registered nurse (RN), is often very challenging to complete due to financial or family constraints, e.g. single parents lacking child care options, unless training institutions offer services to meet these students’ needs. Organizations such as the Health Career Advancement Program (HCAP) play a key role creating the local ecosystems necessary to expand available upskilling options and empower connections between training and career pathways.
Philanthropy also needs to advocate for policy support and worker rights. To create systemic changes, policy change and innovative public-private partnerships will be needed. Recent work by the Brookings Institution highlighted key federal and state-level changes, such as mandated hazard pay, increased Medicaid funding, and expansion of paid sick leave. Furthermore, government-funded training programs can play a key role, such as programs in Washington and Tennessee. New Jersey, with support from Social Finance, is developing a Pay It Forward program, which blends public, philanthropic, and corporate funding into a recycling fund to support training in locally-relevant high-demand sectors. Federally supported Area Health Education Centers (AHEC) also work to connect local support with nationally supported training initiatives. It is time that these “essential” workers are brought out of the shadows and provided with economic security.
4. Enhancing the Current Workforce With Community-Centered and Culturally Competent Care
The engagement of underserved communities and ensuring that individuals with lived experience are at the helm of these initiatives are essential to ensuring the health care system can fulfill its social mission.
To integrate community needs into care systems, we must promote diverse health systems leadership. While 32 percent of patients are BIPOC, members of these communities represented only 11 percent of hospital executive leadership in 2015. This is a reduction from 12 percent in 2013. While 96 percent of surveyed hospitals said they had commitments to diversity, only 45percent said that they had a comprehensive plan for achieving it. Professional groups such as the National Hispanic Medical Association provide trainings for their members to ascend to leadership positions within their hospitals and health systems. In 2019, the American Hospital Association released a Health Equity Toolkit, that includes guidance for measuring diversity and inclusion in hospital leadership and governance.
We must also provide data-driven, community-centered practice that informs programming and cultural training. The evidence is still being formed on the comparative efficacy of various culturally competent health-care practices. Programs such as linguistic matching, involvement of families, and use of community health workers show promise in many settings, and health systems should be intentional about developing a holistic strategy to deliver culturally informed care that fits local needs. One example of innovation is an initiative by the University of New Hampshire’s Institute for Health Policy and Practice to create geographically specific community data reports for hospital CEOs to better inform preventative care priorities and community engagement. Philanthropic funders can play a role piloting and researching community-centered practices for informed care.
The Opportunity for Philanthropy Is Clear and Pressing
Diversifying and empowering the health-care workforce presents an area of significant need. It is also currently an area of significant innovation, carrying the opportunity for systemic change. There are many intersecting objectives for working to improve the health-care workforce: narrowing the racial gap in health outcomes, meeting underserved communities’ increasing need for more health care, and providing economic security to millions of vulnerable, low-wage health employees. Resources and solutions are needed in high-skill positions, such as physicians and dentists, as well as support and vocational roles. State and federal policy is beginning to shift much-needed resources to scale solutions. Traditional institutions, like public university and community college systems, are also showing that they can move the needle on equity and inclusion with policies that center local communities. Philanthropy can play a key role in supporting promising practices, bringing various actors into alignment around health equity outcomes, and catalyzing change across the talent pipeline.
The authors would like to thank the Abbvie Foundation for funding in support of this article. Read more about the Abbvie Foundation’s work here.
Read more stories by Laura Herman, Lily Chhatwal, Ben Wise & Noah Elbot.