

As a healthcare social entrepreneur in India, the magnanimity of the Indian healthcare challenge continues to awe entrepreneurs like myself. There is a dire need for standardized, yet contextual, primary-care enterprises for more than 600,000 Indian villages. But given the complexity of local context and varying disease profiles across different regions, seldom do we ponder learnings from our “Asian” counterparts—the larger Asian healthcare ecosystem that breeds innovation amidst political and cultural diversities.
The term “health systems” paints an abstract picture. We are conditioned to think about healthcare in silos—such as healthcare providers, payors, or patients—and about health outcomes and cost-effectiveness of policies and interventions only intermittently.
Under the aegis of the Health Systems in Asia: Equity, Governance and Social Impact Conference at the National University of Singapore (NUS) presented an alchemic representation of healthcare systems across many Asian countries. Over the four days of the conference, academics, practitioners, policy analysts, and bureaucrats participated and shared their research and learning through nearly 140 oral presentations and 110 poster presentations.
Some of the themes that emerged were:
- Appropriate human resource availability at the last-mile
- Technology enablement for standardized care delivery
- Financing mechanisms with an oscillating balance between tax-financed systems and out-of-pocket expenditure
The World Bank’s Human Development Network Director Timothy Evans showcased Bangladesh as an exemplary example of a country that is making progress in healthcare, citing the 2010 Human Development Report. Performance on health indicators such as immunization coverage, mass mobilization for oral rehydration therapy to manage childhood diarrhea, tuberculosis control, and decline in total fertility rate have been exceptional, given the country’s weak and inadequate physical and human infrastructure.
Most experts attribute Bangladesh’s success to its “pluralistic” outlook, which draws together stakeholders within a health system to collectively and cohesively work toward common goals. Stakeholders within Bangladesh’s pluralistic approach draws on: national and local governments; the private sector, as both formal (high-end secondary and tertiary care / diagnostic centres) and informal (village-level doctors, allopathic and homeopathic practitioners as “first-line” care givers) healthcare providers; the nonprofit sector (primarily to help primary-care service provisioning); and donors.
A receptive health system calls for a congenial and receptive policy environment not only in the context of direct provisioning of healthcare services (as discussed above), but also in other allied sectors such as pharmaceuticals. As an example, in its 1982 National Drug Policy (NDP), Bangladesh strategically subsidized the import of raw material for local generic drug manufacturing, and saw a subsequent surge and exponential growth in the local pharmaceutical market. This established Bangladesh as the first low-income country to develop an indigenous pharmaceutical industry. Even though the success of Bangladesh stands celebrated, the lack of effective regulatory capacity led to minimal compliance with good manufacturing practices, skewed prescription behavior of medical practitioners, and irrational drug usage (prescribing more than necessary) and poly-pharmacy (prescribing too many drugs at one time).
Similar to Bangladesh, China introduced a National Essential Medicines Policy (NEMP) in 1972, and then a reformed iteration in 2009. The three pillars defining this policy were availability, quality, and rational drug usage by medical practitioners. Interestingly, as the Chinese government introduced standards to facilitate rational drug usage—such as additional incentives for physicians, restrictions on varieties of drugs, zero-profit policy, and price reduction—it saw a negative correlation with medical practitioners’ level of enthusiasm and satisfaction.
Another celebrated accomplishment of the Chinese healthcare system is the “barefoot doctor.” Professor Xiulan Zhang from the Beijing Normal University gripped the audience in his talk, “Doctors or farmers? The governance challenge of village doctors in China.” He shared that there are about 1.8 million doctors in China who, in the 1980s, embraced a dual livelihood of farming (as their traditional, rural vocation) and medicine (as healthcare reforms in China encouraged medical skills training at the village level). Around the same time, the Ministry of Health in China introduced a National Examination System to license these village-based doctors; if they passed, doctors gained government endorsement and access to benefits such as pensions. Unfortunately, only 14.3 percent of these doctors have managed to clear the exam; the rest have lost recognition as public healthcare providers, their legal standing, and income.
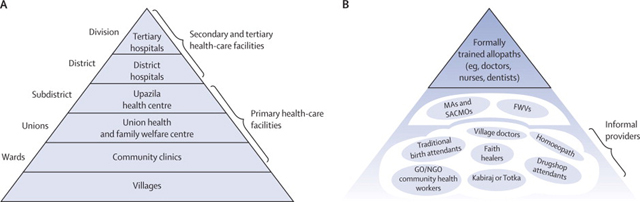 Simplistic depiction of the conventional pyramidal outlook for a health delivery system compared to the pluralistic multi-stakeholder approach in Bangladesh. (Ahmed et al., Harnessing pluralism for better health in Bangladesh, Lancet 2013, 382, 1746-55)
Simplistic depiction of the conventional pyramidal outlook for a health delivery system compared to the pluralistic multi-stakeholder approach in Bangladesh. (Ahmed et al., Harnessing pluralism for better health in Bangladesh, Lancet 2013, 382, 1746-55)
Within the Asian subcontinent, Thailand takes great pride in delivering Universal Healthcare Coverage (UHC)—a 2002 reform of its standard health insurance scheme for formal sector employers—while keeping healthcare spending at less than 4 percent of its GDP. Today, it provides effective healthcare access to its entire population, and notably, it reduced out-of-pocket expenditure from 35 percent in 2001 to 15 percent in 2011. The challenges that daunt Thailand UHC today are an ageing population, medical price inflation, and an increasing demand of healthcare.
Professor Eng Kiong Yeoh from the Chinese University of Hong Kong presented the impact of public-private partnerships on tax-financed healthcare systems across Malaysia, Singapore, and Hong Kong. Singapore lacks comprehensive health insurance, but provides for catastrophic and disabilities coverage for all its citizens. In an attempt to improve the efficiency and effectiveness of its hospitals in 1985, Singapore initiated corporatization of all its hospitals; today it is the defining norm within the country’s healthcare system.
Prime Minister of India Manmohan Singh accorded the highest priority in the 12th Five Year Plan for India, (the government’s plan for 2012 through 2017) to operationalizing Universal Health Coverage (UHC) to all citizens of India, providing them with access to a minimum set of services at the primary, secondary, and tertiary levels.
As India and many other developing nations innovate first-line healthcare delivery (and all its challenges of scale, scope, and diversity), lessons from across the globe can guide our reforms with a view toward contained costs, high-quality healthcare services, and accessibility for all citizens. The pluralistic, multi-stakeholder approach to providing healthcare services has seen varied success across many countries. Three significant pillars within healthcare delivery—specifically for remote populations—are defined as technology, human resource innovation, and innovative financing mechanisms. Making healthcare work at the last mile, fostering a congenial policy environment, and aligning stakeholders are critical as we progress toward a common understanding that meets the expectations of our citizens and complies with acceptable standards of health outcomes.
Read more stories by Zeena Johar.