

 (Illustration by Irene Rinaldi)
(Illustration by Irene Rinaldi)

Deaths of mothers and infants during and after childbirth are tragic and unjust. They are readily preventable and occur predominantly in low- and middle-income countries. The global health community knows how to reduce such deaths, and their near elimination is achievable, if wealthy nations continue to support the right interventions. This is why the United Nations’ Sustainable Development Goal (SDG) 3 targets the reduction of maternal and child mortality.
Since 1990, the United States has played a leading role in the global initiative to lower maternal and child mortality rates. As a result, millions of mothers and children around the world now live healthy, productive lives. Between 1990 and 2015, global maternal mortality rates declined by 44 percent, from 385 deaths per 100,000 live births to 216, according to the United Nations Children’s Fund (UNICEF). Mortality rates for children under 5 years old have fallen by more than half, from 12.7 million in 1990 to 5.6 million in 2016.1
In spite of such tremendous progress, maternal and child deaths are still too frequent. More than 300,000 women died from complications in pregnancy and childbirth in 2015, and almost two-thirds of those deaths occurred in sub-Saharan Africa, according to the United Nations. Approximately 15,000 children continue to die each day, often from preventable causes such as pneumonia, diarrhea, and malaria. Proven lifesaving interventions are effective only if financial support is available to disseminate them and increase their scale. But according to the World Bank, the SDGs related to maternal, newborn, child, and adolescent health face an annual funding gap of $33 billion.2
Official development assistance (ODA) from wealthy countries continues to play an important role in achieving the SDGs—particularly in fragile and conflict-affected states. But it is no longer the dominant source of capital flowing to developing countries. Today, more than 80 percent of US money going to emerging and developing economies takes the form of foreign direct investments, remittances, and private philanthropy.3 Given this new development landscape, financial innovations offer the potential to close the $33 billion gap.
The United States should use its position as the largest bilateral donor in the world to catalyze investments from other sources. Specifically, development impact bonds (DIBs) offer a promising way to use innovative finance to eliminate maternal and child mortality. The main goal of a DIB mechanism is to attract private capital to social projects, and for private investors to earn a profit if the social outcome is achieved. The DIB structure ensures that governments, donors, or other outcome funders in international development projects will pay for interventions only if an independent evaluator deems them successful—hence the alternative moniker for impact bonds: “pay for success.” By offering a potential profit to investors, as well as guaranteeing the security of impact for outcome, DIBs have the long-term potential to attract more funding and participation to international development.
This article is intended to contribute to the evidence base on DIBs. Its core analyzes two case studies of DIB projects in the field of maternal and child health and survival. These are relatively new projects, launched in the past two years, and my analyses are based on reviews of program evaluation documents and in-depth interviews with DIB participants, donors, and experts. Their experiences and challenges may help further the understanding and use of DIB financing for development interventions.
A Focus on Outcomes
DIBs are just one among many innovative finance tools that donors and developing countries’ governments are now piloting and testing to address social and environmental challenges. Unlike much current international development funding, DIBs focus on outcomes, rather than inputs or outputs. By guaranteeing that outcome funders spend resources only on successful projects, DIBs require rigor and focus on the impact of development.
Because the DIB model is new, limited evidence of its effectiveness is available. As of December 2019, 11 contracted DIBs existed globally, according to Brookings Institution data. They are modeled after social impact bonds (SIBs), which are designed to overcome the challenges governments face in investing in social innovations. They mitigate the risks of failure and bring in investors that provide flexible funding to programs that seek to respond to the needs of vulnerable groups.
The British NGO Social Finance UK developed the SIB model. It launched its first SIB in 2010 to help reduce recidivism in Peterborough, United Kingdom.4 Whereas SIBs have governments as the primary outcome payer, DIB outcome payers often include an international donor.5 While still in their early days, SIBs have shown some evidence of success in the United Kingdom. The Peterborough SIB focused on reducing recidivism and succeeded according to independent evaluators.6 To date, almost $400 million has been invested into more than 100 SIBs in 19 countries.
USAID has supported using DIBs as a way of finding new and alternative sources of funding for development. Administrator Mark Green launched USAID’s first DIB in November 2017 in the state of Rajasthan, India, to support maternal health-care facilities there.
“This results-based financing mechanism … takes a business approach to development while still targeting basic needs like improving the quality of care and private facilities,” Green said when the DIB launched. “By leveraging the assets and skills of a diverse group of partners across the public and private sectors, we are stretching our investments further while saving more lives.” 7
Six Stakeholders
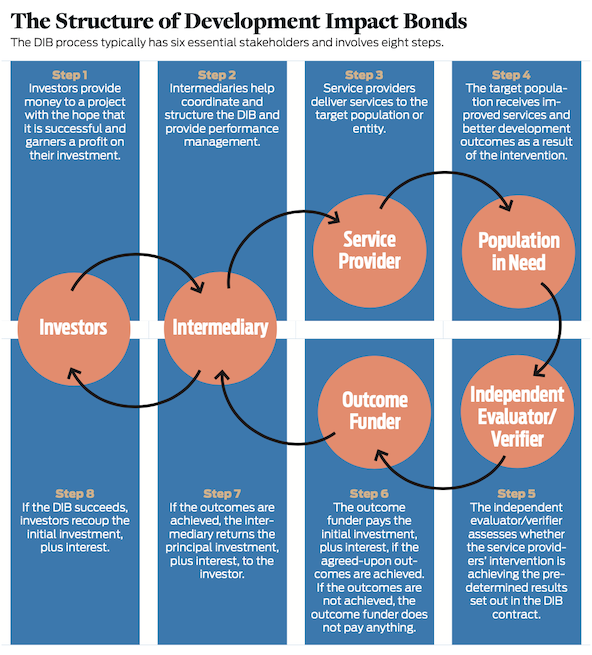
DIBs can take a number of forms, depending on the local circumstances, type of intervention, array of stakeholders, and other variables. While the purpose of DIBs is to attract private finance into development projects, other players can serve as investors and outcome payers, including donor agencies, multilateral organizations, and philanthropists. Generally, DIBs consist of an outcomes-based contract involving six essential stakeholders:
- Investors provide the initial investment and ongoing project capital to cover DIB costs. Since outcome funders make payments only if predetermined results are achieved, investors bear the risk of losing their money if the outcomes stated in the contract do not materialize, but earn a profit if they do. The alignment of investors’ financial returns with the achievement of results means investors have a strong incentive to support effective performance management. Philanthropic foundations, particularly the philanthropic arms of private investment funds, have often taken the lead as investors. Early DIB investors include the UBS Optimus Foundation, the Bridges Impact Foundation, and the Silicon Valley Social Ventures Fund (SV2).
- Intermediaries (or project designers or DIB managers) help bring together stakeholders and provide performance management and analytical support. The intermediary oversees the delivery of agreed-upon outputs and outcomes by continuously analyzing service delivery and outcome data and by guiding the work of service providers, including shifting resources as needed. Investors typically pay the intermediary an annual fixed fee for service, alongside a performance-related fee.
- Service providers implement the DIB intervention. While only one service provider may exist, the complexity of DIBs often requires multiple, coordinated service providers, such as an international NGO working with a local implementer.
- The population in need is the target population for the DIB. In the two case studies featured in this article, target populations include pregnant mothers and infants in regions that lack adequate health facilities and health-care staffing.
- Independent evaluators (or independent verifiers) determine whether the project has achieved its predetermined metrics and whether payouts to the investor are due from the outcome funder.
- Outcome funders are typically donors or multilateral agencies (for example, USAID or the World Bank) that pay the investors if and when the previously agreed-upon project outcomes materialize. The outcome funder is not involved in program delivery but provides the funding to pay if the DIB goals are achieved. Outcome funders also typically pay for the project evaluation or verification. The outcome funder receives regular updates on the intervention’s progress and commits to paying only for independently verified results or outcomes that the contract sets.
To get a better sense of how DIBs can bridge the financial gap preventing the reduction of maternal and child mortality in the developing world, let us review the two DIBs specifically addressed to finance this outcome.
The Utkrisht Impact Bond
In 2012, India co-convened the Child Survival Call to Action with the United States and Ethiopia. The initiative, a collaboration with UNICEF, brought together 700 leaders from government, business, religion, and research to reenergize the global effort to end preventable child deaths. Following the gathering, 178 governments—as well as hundreds of civil-society, private-sector, and faith-based organizations—pledged to end preventable deaths among women and children.
India has taken the lead in increasing budget allocations for and strengthening policies to support maternal and child health. In recent decades, it has made impressive strides. Between 1990 and 2015, the number of under-5 deaths in India decreased by 62 percent, from 3,357,000 in 1990 to 1,201,000 in 2015, according to UNICEF. Despite such progress, India still accounts for the largest number of deaths among that age group of any country in the world, and 20 percent of the global total. Within India, the state of Rajasthan has one of the country’s highest maternal and neonatal mortality rates: An estimated 80,000 babies die there every year. While India’s overall newborn mortality rate is 28 per 1,000 births, in Rajasthan the rate is 47 per 1,000 births.8 Similarly, India’s overall maternal childbirth mortality rate is 178 per 100,000 births, while Rajasthan’s is 244 of every 100,000.
As with India as a whole, Rajasthan has made progress in reducing maternal and child mortality. In part, the government of Rajasthan has successfully encouraged pregnant women to deliver in maternal care facilities, instead of at home. While most mothers use public facilities, about 25 percent of all births in Rajasthan occur in private hospitals that are filling a gap in service provision. But unlike public hospitals and clinics, private facilities in Rajasthan are not required to meet government quality standards to be considered for reimbursement. Births in maternal health-care facilities will not improve outcomes if those facilities are not high quality. Consequently, perhaps, moving mothers to maternal care facilities did not result in the expected improvement in maternal and newborn survival outcomes. Public-health experts working in India have found that this discrepancy is at least partially due to the state’s lack of quality facilities, which will require investments to improve.
The Utkrisht Impact Bond, the world’s first health-impact bond, officially launched in November 2017. Named after the Hindi expression for excellence, it seeks to improve and standardize the quality of maternal care in Rajasthan’s private health-care facilities. The project will take place over three years, with a projected total investment of $9 million.
The DIB’s broad goal is to provide incentives for private facilities to be accredited through the government-approvedhealth-care facility certification process. This certification will be granted only when private health-care facilities are upgraded to meet specific maternal care quality standards. The project’s implementing partners will guide the targeted private health-care facilities through quality improvements to meet these government standards, as well as assist them with the application process.
Over the course of the DIB, the intervention will cover a total market of 68 million people across Rajasthan, affecting up to 400,000 women and newborn babies, and may save the lives of approximately 10,400 women and children (based on an anticipated 20 percent reduction in newborn mortality).9 These are not outcomes that the DIB will measure but are projected impacts if the DIB realizes its outputs of improved maternal care facilities.
The Utkrisht DIB includes components intended to ensure that the government will sustain the project’s impacts, if achieved. Rajasthan’s Ministry of Health signed a memorandum of understanding to invest in and scale up the partnership if the independent evaluator deems the pilot program successful.
USAID and Merck for Mothers,10 the chief outcome funders, are collectively providing up to $8 million. Joe Wilson, former senior advisor for innovative finance at USAID, says this DIB is part of the agency’s growing emphasis on paying for outcomes. “Performance-based finance is going to be a critical piece of what [USAID administrator Mark Green] does,” Wilson says. “[DIBs] are going to be one of the tools in the tool box to drive an efficiency conversation.”
Merck for Mothers has a history of working on maternal health in Rajasthan. It supported the DIB as a way to ramp up its previous work in this region and sector. “What better way to measure actual results than to have a pay-for-performance type of structure?” Scott Higgins, of Merck for Mothers, says. “You’re putting your money where your mouth is.”
The UBS Optimus Foundation (UBSOF) is Utkrisht’s chief investor, providing 80 percent of the $4 million up-front working capital that the project needs. UBSOF is also the investor in the first-ever DIB, launched in Rajasthan in 2015 to improve girls’ education. Maya Ziswiler, head of social and financial innovation for UBSOF, said the organization drew on its experience with the first DIB in designing Utkrisht. “In the first DIB, we had one service provider,” Ziswiler says. “In the new DIB, we have two service providers, which can be more efficient in delivering the outcomes. Part of any DIB is delivering outcomes in a cost-efficient way, so working with several service providers is a step forward.”
The two service providers—the international and Washington, DC-based Population Services International (PSI) and Hindustan Latex Family Planning Promotion Trust (HLFPPT), a regional organization—and the project intermediary, global consulting firm Palladium,11 will provide the remaining 20 percent of investment capital. Through its work with development partners, PSI identified a set of proven interventions to prevent maternal and infant deaths that might interest potential outcome funders and impact investors. This approach led PSI to work with USAID and then Palladium, which was exploring its own impact bond in Rajasthan with Merck for Mothers.
HLFPPT, with help from USAID, has worked with private health facilities in India for more than a decade. Currently, the social enterprise has a network of 800 private providers across five Indian states. In Rajasthan, HLFPPT has worked with Merck for Mothers to move the private sector to address maternal- and child-health issues. With a focus on maternal and newborn health, the Utkrisht DIB is a continuation of previous partnerships between USAID, HLFPPT, and Merck for Mothers.
Palladium helped design the DIB and is also the DIB performance manager. The firm has been involved in private-sector development for more than 50 years. “Impact bonds really spoke to us—the transparency, the engagement,” former Palladium head of innovative impact financing Peter Vanderwal says. “It makes sense for our company to take the leap and to commit to being a partner … because we have the pockets, the risk appetite, and a portfolio of projects across the world.”
The Cameroon Newborn Development Impact Bond
The world’s second-ever health-focused DIB is taking place in Cameroon. As with India and Rajasthan, the West African nation has made progress in reducing early childhood deaths but still suffers from excessively high rates. In 2015, Cameroon had an under-5 mortality rate of 88 per 1,000 live births (71,000 total deaths), according to UNICEF. While this represents a 36 percent decline from its 1990 rate, Cameroon is still burdened with Africa’s 19th-highest rate of under-5 mortality.
Newborns—children less than 28 days old—face particular mortality challenges and respond to specific interventions. In Cameroon, the newborn mortality rate is 26 per 1,000 live births, according to World Bank and World Health Organization data. Among these newborns, 60-80 percent of deaths are due to low birth weight (LBW). In addition to being the leading causes of newborn death, LBW and preterm birth can lead to high incidences of health complications. Even when a child survives, these complications can create additional negative health outcomes, many of which can last into adulthood.
Kangaroo Mother Care (KMC) is a cost-effective intervention suited to low-resource countries such as Cameroon. Developed in Colombia during the 1970s, KMC was designed specifically for preterm infants in countries where incubators were either unavailable or unreliable and is modeled after the way marsupials carry their young. It prescribes long periods of skin-to-skin contact between child and caregiver, along with exclusive breastfeeding. Newborns and infants who receive this type of care are typically discharged from the hospital earlier. It has also been shown to effectively reduce both infant mortality and hospital-acquired infections.12
Kangaroo Foundation Colombia (KFC) launched in 1994 to promote KMC and has trained more than 75 teams from 35 countries. KFC brought the technique to Cameroon in 1998, through training pediatricians and nurses from the Laquintinie Hospital in Douala. This introduction led to the creation, in 2015, of Kangaroo Foundation Cameroon to implement KMC in Cameroon. But the effort to boost access to KMC in Cameroon has remained limited because of financial and implementation barriers, including inadequate hospital infrastructure, equipment, and protocols; lack of ongoing KMC training and support for personnel; and insufficient awareness of KMC.13
Cameroon’s Ministry of Public Health has a five-year action plan to improve newborn health by expanding KMC to reach more preterm and LBW infants. To support this plan, the ministry became the outcome funder for the Cameroon Newborn DIB, which launched early in 2019 to invest $2.8 million over three to four years. The Cameroon Ministry of Public Health has committed $2 million, while a second outcome funder, Canadian INGO Nutrition International, has committed $800,000.
The effort will promote KMC in up to 10 hospitals across four or five regions and will reach an anticipated 2,200 LBW children by 2021. It seeks to improve intermediate outcomes, such as the reduction of severe infection, like sepsis, and above-average weight gain for infants, and has the ultimate goal of significant and verifiable improvements in LBW infant health. It also aims to integrate high-quality KMC into Cameroon’s public health-care system to ensure its long-term sustainability and expansion to hospitals nationwide. “Using a DIB, we are sure of attaining the results,” says Dr. Martina Baye, coordinator of Cameroon’s national program to combat maternal newborn and child mortality at the Ministry of Public Health. “It’s not like other funding, where you look for results that you may or may not have.”
Grand Challenges Canada (GCC) stepped in as the investor, although it originally sought to play the outcome-funder role. GCC is funded by the Canadian government and other parties and supports development innovations in low- and middle-income countries.
“Our mandate for the last seven years has been how to scale the most promising ideas out there to overcome the largest health challenges,” says GCC co-CEO Karlee Silver. As Silver and GCC reviewed their portfolio for potential DIB projects, the Kangaroo Foundation Cameroon’s work stood out for its strong evidence base. “KMC has been known for ages. There’s lots of evidence behind it on the mortality front, a unique amount of evidence,” Silver says, “but there’s a real block in terms of how to actually scale it. Those were our two starting points.” 14
One of the major reasons Cameroon’s KMC work was selected for a DIB intervention was the strength of the evidence supporting its efficacy. The service providers for the Cameroon Newborn DIB—Kangaroo Foundation Cameroon, Kangaroo Foundation Colombia, and Laquintinie Hospital—have experience with KMC. Kangaroo Foundation Cameroon will lead the training in partnership with Cameroonian government hospitals.
The Cameroon DIB has two main project intermediaries: MaRS Centre for Impact Investing—a Toronto-based consultancy that previously advised GCC—and Social Finance, a UK-based nonprofit advisory organization that developed the first impact bond in 2010. Given its previous partnerships with GCC, the MaRS Centre recommended a DIB to grow the GCC-supported KMC work in Cameroon. “[GCC was] looking to scale this through an outcomes-based, data-driven, pay-for-success model,” MaRS Centre senior associate Kia Kavoosi says. “KMC came to the top because of its strong evidence base. It’s quite important in this model to have that.” The DIB design team subsequently brought on Social Finance, which also had a previous relationship with GCC and the MaRS Centre, for its history with pioneering impact bonds.
Challenges
Although DIBs are young, development organizations and impact investors can learn a lot from these efforts. Representatives of the parties involved in both DIBs cited three challenges to address if DIBs are to expand.
The bespoke nature of DIB formation | In both efforts, the lack of a DIB template led to an onerous DIB design process—a problem that many of the stakeholder organizations’ lack of experience operating within a DIB structure, particularly in regard to project finance, contracting, and legal frameworks, compounded.
“We are trying to go into these [DIBs] with a system and a process that has been established for something that is very different,” Marcie Cook of PSI says. Cook’s PSI India colleague Pritpal Marjara agrees that building the DIB from scratch was laborious. “We spent quite a bit of time developing the theory of change,” he says. Peter Vanderwal of Palladium, which invested years helping design the Utkrisht impact bond, says the costs of starting the design from scratch were significant. “We tried as much as possible to create templates so that [we had] the potential for replicability,” Vanderwal says. “I don’t believe we achieved that.”
The Cameroon DIB stakeholders echoed these sentiments. “The field is so nascent that it’s almost starting from scratch … every single time,” Silver says. “[There isn’t] a model where they can pull things off the shelf.” Dr. Martina Baye, of the Cameroon Ministry of Public Health, echoes the long timeline required to create a DIB. “It takes a lot of meetings,” she says. It also requires detailed mutual understanding of financial, legal, and contractual issues.
Using a DIB, we are sure of attaining the results. It's not like other funding, where you look for results that you may or may not have.
Much of this design and consensus-building work falls to the project intermediaries—in this case, Social Finance UK and the MaRS Centre. “Any product that is new [includes] transaction costs and time to launch,” Kavoosi says. A lot of the up-front work to design the DIB is done pro bono, “to subsidize what would typically be more efficient … for a more mature market.”
Aligning DIB project stakeholders’ incentives and outcomes | DIBs bring together an array of parties from philanthropy, the private sector, bilateral and multilateral donors, and officials from developing countries. But because of the specificity that designing DIB outcomes and payments requires, aligning organizations with differing goals is hard. “Everyone cares about the mortality and morbidity of these children, but tying them to payments becomes extremely difficult when you have a lot of attribution problems and confounding variables,” Kavoosi says.
“You’re going to have to be flexible in order to make the … parties happy,” PSI’s Cook says about the Cameroon Newborn DIB experience. Much of the negotiating centered on defining maternal-quality-of-care indicators and metrics.
Aligning organizational education and support | The Cameroon Newborn DIB team said that in some cases, using the DIB mechanism required extensive education and awareness raising to garner organizational support. “There’s a lot of conversation [about] why we would use [a DIB] versus [a more traditional grant],” GCC’s Silver says. “That [includes] a lot of proof points on how a DIB can transfer responsibility … to the government.”
Others echoed this challenge. “[It takes time] getting people over the learning curve,” Kavoosi says. “Accountants are not trained in results-based financing,” Erik Nielsen, formerly of Nutrition International, adds. “You need lawyers to provide guidance and advice.”
Some of the Utkrisht DIB stakeholders found that the leaders of other stakeholder organizations were tentative about joining the impact bond team. This hesitation slowed the formation of the legal, financial, and contractual negotiations needed to create the bond. “Public- sector agencies are the most risk-averse,” Palladium’s Vanderwal notes, but he finds that the private sector also has difficulty with DIBs’ large start-up costs and lack of structure. “It’s not something that most companies would have the appetite for,” he says. “We’ve got to have leadership from government and leadership from donors. They’ve got to be willing to put in the effort to understand what’s needed to structure one of these.”
Not everyone agrees with these sentiments. Leaders at Merck for Mothers say it was not difficult to build organizational support for the DIB, even though it was their first impact bond and they had no previous relationship with Palladium. “Merck is into taking risks, so the question of leadership supporting this has never been an issue,” says Scott Higgins, Merck for Mothers’ director of operations.
Lessons Learned
DIBs are not intended to replace traditional bilateral or multilateral assistance; they merely seek to add new funding sources to address social and economic needs in developing and developed countries. The experiences of the Utkrisht and Cameroon DIBs reveal several ways to make DIBs a more streamlined, cost-effective, and scalable development finance option for the United States and other donors.
Essential criteria must be in place before the decision to launch a DIB | Project advisors must first analyze whether the cause or idea is suitable for a DIB. According to Social Finance’s Nita Colaco, important questions include “Is there a clearly identifiable target population? Are there clearly measurable outcomes on which payments can be made? Is private financing required?” If the proposed project does not meet these and other basic criteria, a DIB might not be the best choice, Colaco says.
DIB outcomes must be measurable | Utkrisht DIB stakeholders say the ability to identify and measure outcomes was crucial. Joe Wilson, formerly of USAID, says that DIBs must be “measurable, costable, and quantifiable—the availability of quality data is essential.” Given the complex structure of DIBs, metrics must be established early in the DIB design.
Time and energy for stakeholder education must be budgeted at the outset | Participants in both DIBs emphasized cultivating understanding among senior decision makers of stakeholder organizations. “There’s a general level of education and awareness needed before you even start talking about what the opportunity is,” GCC’s Karlee Silver says. Dr. Martina Baye added that an important part of Cameroon’s involvement in the DIB required persuading government decision makers. “The very first thing to be done was to sensitize the minister of health and other stakeholders … to understand why they should invest through [a DIB],” she says. “Decision makers need to understand what this means. … They want to know the money they are putting on the table will actually bring results.”
Early-adopter DIB stakeholders are not motivated solely by profit | At this early stage of piloting and testing DIBs, participating organizations and individuals must be motivated primarily to make an impact and to innovate, not to prioritize profit. “[You need] a group of people who care primarily about the social impact, no matter whether you sit on the investor side or the outcome side,” GCC’s Karlee Silver says. “You have to care that more low-birth-weight newborns in Cameroon are going to get quality KMC. It’s not enough of a financial bonus that a returns-only investor would be interested.”
Just as it was a leader in the creation of the Global Financing Facility, the United States could also lead the creation of a DIB hub.
Costing | While closely related to the importance of outcomes measurement, costing deserves its own discussion in the context of DIB creation. A project in which investors are confident must link potential impacts to costs. The impact evidence base and the cost of those impacts are crucial to creating a strong DIB framework. “From an NGO perspective, we had to do a lot to really understand our costs and to be able to present them in a way that we don’t [typically] do,” Marcie Cook of PSI says. “In a traditional contract, you are not necessarily rewarded for being more efficient at the end of the year.”
Cook says that one reason PSI chose India as the site for its DIB was a robust evidence base that allowed it to “determine outcomes from inputs and costs that enabled it to be potentially aligned with how an investor would think about ROI.” Good impact measurements and costs are essential building blocks for a strong DIB project model.
Joe Wilson, formerly of USAID, says he spent six months at the beginning of the DIB process working to identify both costs and the right type of intervention. “[We were] working with PSI and others on where [outcomes-based finance] is appropriate, and where it’s not. What can we measure? What can we cost out?” Wilson says. “Having more clarity around that is the first step. If you have no idea what something is going to cost you, you can’t possibly push it, particularly in this environment, where we have really tight budgets. At the end of the day, if you can measure it and cost it, you are well on your way.”
Recommendations
I reviewed these two DIBs extensively in my role as director of policy research at Save the Children USA, the US branch of the 100-year-old, UK-based international organization dedicated to improving child welfare worldwide. I offer four recommendations for improving and growing DIBs.
First, develop a central DIB platform. Since DIBs are a nascent finance tool and involve a complex and new array of development stakeholders, they need a more coherent system for aligning varied interests. Specifically, the sector needs a central DIB platform where entities interested in taking on one of the various DIB roles can coalesce. These entities may include investors, outcome funders, intermediaries, evaluators, and local and international implementers.
Given its leadership in global maternal and child health, the United States can use its convening power to assess the nature and utility of a global platform to facilitate DIB supply and demand. This country is well positioned to convene stakeholders on the issue. Just as it was a leader in the creation of the Global Financing Facility, the United States could also lead the creation of a DIB hub.
“More and more explicitly, positive impact is around coalitions,” Peter Vanderwal of Palladium says. “You need different players to bring different pieces of the jigsaw together.” Maya Ziswiler of UBS believes a global fund is the future of DIBs: “We are hoping to … move from small transactions to larger transactions, to a fund where you are pooling outcome funds … where you can attract more mainstream investors.”
Second, convene and educate internal and external stakeholders. While a central platform is a long-term tool to mainstream DIBs, a short-term need is to educate potential stakeholders about what DIBs are, as well as about where, how, and when they can address the maternal- and child-health goals of donors, philanthropists, and others. Many misconceptions still surround DIBs, and these need to be demystified for relevant parties to adopt DIBs more broadly. USAID’s focus on innovative finance makes it ideal to convene DIB knowledge exchanges, both within the US government and with its global donor peers.
For example, a pay-for-success interagency group focused on domestic impact bonds within the US government already exists. As the leading US development agency, USAID should draw from its experience to educate both US government and international donor community practitioners on how to apply DIBs to foreign-assistance challenges. Many of the stakeholders interviewed for this report are still learning about DIBs but became involved because of their eagerness to participate in an innovative development finance project.
“We are not there yet, but we are learning how DIBs are structured in terms of the risk, in terms of shifting the accountability to the results and not to the process,” Pritpal Marjara of PSI India says. For his part, Joe Wilson, formerly of USAID, says, “Having a little bit more collaboration and communication between investors and outcome funders up front, and then allowing them to communicate that to the entire world of implementing partners, is probably the best starting point.”
The Brookings Institution has disseminated multiple DIB research reports that emphasize educating both potential outcome funders (such as donor agencies, foundations, and governments) and private-sector investors. If DIBs are to grow and achieve global reach, these two stakeholder groups must be better educated about when DIBs are an appropriate funding option.
Third, increase the evidence base on what works for DIBs. DIBs for maternal and child health need a more substantial evidence base, and more learning on DIB formation and field impact is necessary across the board. DIBs are in the early stages of implementation and evidence building. Ensuring rigorous program evaluations and disseminating evidence and lessons on the formation process and outcomes will be important in strengthening the DIB model and building confidence among risk-averse organizations. “Funders want to support interventions and service providers that have a record of achieving outcomes,” says Emily Gustafsson-Wright of the Brookings Institution.15
Fourth, institutionalize innovation within USAID. The US government must signal its commitment to innovation in maternal and child health. To accomplish this goal, the administration should provide high-level political support for the Center for Innovation and Impact (CII). Established in 2012, the CII resides in USAID’s Global Health Bureau and invests seed capital in promising ideas, using a business-minded approach to the development of health interventions. Over the past five years, CII has attracted more than $300 million in investment capital on an annual budget of roughly $5 million.16 USAID should entrust CII and direct the various USAID missions and program offices within the Global Health Bureau to devote a small percentage of their annual funding to programs that use CII’s development finance expertise. Building and strengthening CII’s consulting work within USAID can help integrate its expertise throughout global health programs.
Reducing maternal, newborn, and child mortality involves immense challenges. As domestic revenue mobilization grows, countries can increasingly finance their own maternal- and child-health system enhancements. However, until developing nations become fully self-sufficient, other financial mechanisms must fill the gaps in supporting maternal and child survival. DIBs are a potent tool to meet this challenge.
Read more stories by Andrew Wainer.