

 (Illustration by Øivind Hovland)
(Illustration by Øivind Hovland)
Why do some health collaboratives flourish while others decline or fail? Consider the following two real-life examples.
In the Pacific Northwest, four counties were struggling to meet the health-care needs of residents who lacked adequate health insurance. Patients were often unable or reluctant to seek care when they needed it. Many could not afford primary and preventive care, and when they did get care, it was usually urgent and sought in emergency rooms. Patient health suffered, and the cost of medical care was high.
A senior leader from one hospital, a physician who had credibility in the medical community, convened leaders from major local employers, hospitals, two primary care practices, and a major insurer. Together these leaders formed the Pacific Multi-County Health Collaborative,1 mobilized volunteer health-care workers to treat the underserved, and created a new community health center to provide affordable primary and preventative care. Their early efforts included the improvement of prenatal care for pregnant women, a joint investment in a trauma care center, and an electronic medical records system to enable providers to share patient information. These projects built momentum and a track record of successful collaboration that reinforced the partners’ willingness to collaborate.
Meanwhile, across the country in a Northeastern city, the public health department convened eight leaders to discuss how to provide care for the underinsured members of the community. The resulting New England Healthcare Collaborative included three hospital CEOs, plus senior leaders from a mental-health clinic, a children’s health center, and a major private insurer. The group met monthly for two years, but significant conflicts arose among members about whether their purpose was mainly about “sharing the burden” of providing care without adequate reimbursement, or whether they had a broader, health-promotion mission. They produced a high-quality assessment of local health-care needs, but without agreement on a purpose, they never implemented any significant initiatives to address those needs. Their sense of accomplishment was low, and trust among group members consequently eroded. They continued to attend meetings mainly to ensure that no decisions that could affect their organizations were made without their knowledge.
LISTEN: Hear more from these authors about what makes health and health-care collaboratives thrive on Spring Impact's Mission to Scale podcast.
As with many other complex social problems, providing excellent care to everyone cannot be solved by one organization or one sector alone. Health collaboratives, composed of public, nonprofit, investor-owned, and community-based organizations, have emerged in many regions of the United States to improve community health and health-care delivery. When they work well, they draw on the combined strengths of their members to address a region’s unmet health-care needs, reduce costly duplication of programs and services, improve social determinants of health, and give marginalized groups access to care.
But not all health collaboratives in the United States live up to their potential. While some grow and sustain themselves over time, others suffer diminished capacity and impact, or dissolve altogether. What explains the difference between success and failure? We examined the experience of 19 health and health-care collaboratives that we selected carefully for the variety they demonstrated in developing collaborative capacity over time. The examples varied widely by geographic location, by the economic status of the community served, by the life span of the collaborative, and by its role in the community. Projects also differed in funder involvement: 13 initiatives were guided by frameworks developed by nonprofit and government funding organizations, such as Project Access, the Institute for Healthcare Improvement’s IHI Triple Aim initiative, and the Beacon Community Program, while 6 were not explicitly organized around funder-driven frameworks.
Our interviews, background research, and data analysis found that high-impact collaboratives all share the characteristic of developing and growing collaborative capacity—i.e., the ability and motivation of parties to work together to produce desired community-level outcomes.2 Collaborative capacity is a community-level resource that is built or depleted as a consequence of how members of the collaborative act (or do not act) in pursuing a joint goal. This kind of capacity is critical to tackling so-called “wicked problems,” 3 or social challenges that are difficult to solve because they are driven by multiple, contingent, and conflicting issues and are beyond the control of any one institution.4
How is collaborative capacity developed? We know from prior research by others that multiple drivers can influence outcomes. But scholars who study collaboratives have yet to untangle how the dynamic interactions of multiple drivers over time combine to produce successful or unsuccessful outcomes, let alone offer guidance to leaders of collaboratives about which moves to make and in what order. Our research takes these next steps.
We developed an initial framework, drawing on elements from the existing literature on collaboratives and our own thinking about how these elements interact in ways that shape the collaboratives’ trajectories. We then modified and validated the framework through our research into the 19 collaboratives.
The dynamic framework for collaboratives that we ultimately formulated integrates our insights into how collaborative capacity can develop and produce effective impacts. Our research identified a small number of essential strategic moves to make at the beginning of a collaborative’s formation to set it up for success, and to make subsequently to build positive momentum over time and avoid tailspins. Likewise, we identified negative dynamics to avoid. Our work is most relevant to health collaboratives, since they were the focus of our research, but we believe that many of our findings also apply to collaboratives working on other complex, systemic environmental, social, and economic issues that no one organization or one sector of society can solve.
Framework for Successful Collaboration
Our dynamic framework for successful multistakeholder collaboration is based on the premise that collaborative capacity develops over time as part of a closed-loop process in which capacity enables a collaborative to have impact, and that impact in turn motivates investment in further capacity-building. Collaborative capacity, which enables a collaborative to take action, arises from a combination of its participants’ motivation and their ability to work together effectively. The actions a collaborative takes have impacts that participants perceive, and these impacts then affect both their motivation to participate in the collaborative and the collaborative’s ability to take action in the future. Such feedback loops enable collaborative capacity to grow over time.
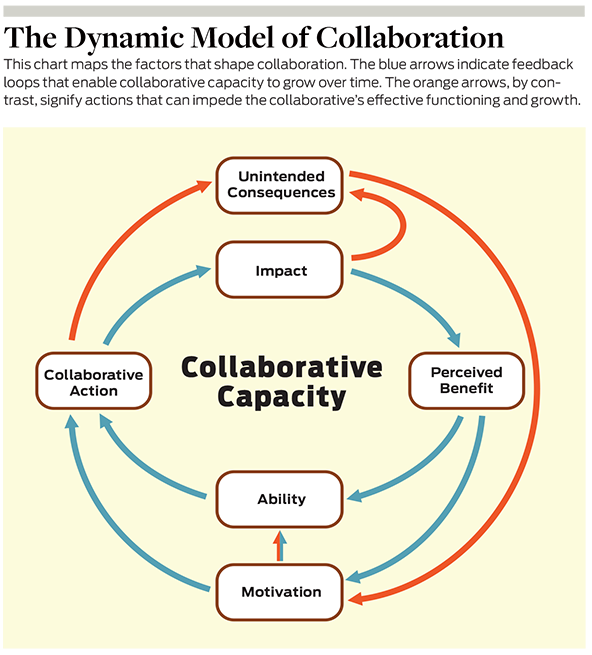
However, a collaborative’s actions may also set off unintended consequences that form closed loops of their own and can impede the collaborative’s effective functioning and growth. These impediment loops can cause a collaborative to stagnate or even go into a tailspin.
We found that each of the factors in this model have their own direct influences on other factors, and that each factor is in turn influenced by sets of variables that leaders must manage as they grow their partnership. Of central importance to stakeholders’ motivation to collaborate is whether the stakeholders have a shared purpose, a collective definition of the problem to be solved, a vision and strategy for change, shared values about a positive future, and a unified belief about how collaborative work should be accomplished. Trust that others will collaborate—the degree to which members confidently expect that other stakeholders will work toward mutual benefit—is another critical influence on motivation.
Several components interact to influence stakeholders’ ability to collaborate and have impact. First, a collaborative must achieve the right breadth of vision to drive meaningful change. Breadth of vision describes the extent to which stakeholders desire change and believe it is possible. A narrower vision can enable rapid progress and keep members optimistic about their ability to make an impact. However, a too-narrow vision runs the risk of ignoring vital contextual issues, causal factors, and constraints; producing only limited accomplishments; and distracting members from pursuing more fruitful, though difficult, changes that improve the population’s health and access to health care.
Second, a collaborative needs sufficient infrastructure to enable progress on interdependent tasks. Researchers often refer to this infrastructure as a “backbone organization.” Such organizations provide critical administrative support to their collaboratives, convene meetings, coordinate actions by stakeholders, and help assure that the collaborative is making progress toward its objectives. The backbone organization or other administrative structure needs the right management and staffing to support how the effort is governed; how key information is collected and synthesized; and how joint tasks are defined and coordinated. Backbone organizations are essential to achieving collective impact—what John Kania and Mark Kramer define as “the commitment of a group of important actors from different sectors to a common agenda for solving a specific social problem.” 5 Developing infrastructure support depends on participants’ willingness to invest resources in the initiative in ways that are equitable for members without becoming overly reliant on a single funding source.
Third, a collaborative needs appropriate reward structures. Members need to see a benefit to invest further in the collaboration. They need to perceive that positive outcomes for the community are positive outcomes for themselves.
Closed-loop causal relationships can positively reinforce the development of collaborative capacity and promote its growth. Collaborations that produce measurable impact also increase the benefits members perceive from collaboration and motivate greater participation. Measurable impact leads to other positive effects that enhance the ability to collaborate, such as the potential to pursue new sources of funding or build more infrastructure, which enables yet further collaboration and accomplishment.
One long-standing collaborative in the southeastern United States illustrates these relationships. The Peachtree Regional Health Council (the Council) began as a cross-organization collaborative to help indigent community members access care. The Council included the commissioner of public health, social services agencies, three hospitals, a community health center, and a university-affiliated health policy institute. The Council defined a role for itself as both a think tank and a steering group whose leadership role was to imagine a suite of interrelated initiatives and to mobilize people and funding to achieve them. The Council quickly organized its members to launch initiatives not just related to increasing access to care but also involving and empowering local citizens to improve health in the community. With a handful of projects underway, jointly funded by the members of the partnership, the Council quickly demonstrated success to other local organizations. Its ability to get things done, and in a way that involved citizens, attracted additional partners in and resources from organizations with similar values. This track record led to increasing confidence and efficacy resulting in many initiatives that had an impact on the community’s access to health care and involvement in health promotion.
Over time, the Council derived strength from resources invested by the partner organizations and built further support by gathering and sharing data about the impact of its projects. It provided the backbone support that the many initiatives under the Peachtree umbrella needed. Guided by its purpose as an incubator of a portfolio of projects, this collaborative continues to be an active leader of community health initiatives.
Like all dynamic processes, these relationships can also influence one another adversely in reinforcing feedback loops, initiating and amplifying downward spirals. Failure to produce impact can weaken stakeholders’ motivation to ensure continued participation.
Four Possible Trajectories
The collaboratives we studied evolved along a range of trajectories. A number exemplify how the right strategies can play out and result in sustained growth in collaborative capacity and impact. Others illustrate how the failure to execute those strategies and/or experiencing impediments to growth can block a collaborative from developing or cause it to stumble after early success.
The first trajectory never gets off the ground. This can arise from a lack of initial conditions that promote either motivation or ability to collaborate. One collaborative in our study, the Midwest Two Hospital Cancer Care Collaborative, failed because it never built the trust it needed to launch. A group of physicians in a small Midwest city pulled together leaders from the two local hospitals and others from the medical and business communities to see if they could agree to build a treatment center jointly, rather than compete and cause spending to escalate dramatically.
However, the effort was troubled from the start. The hospitals had no history of collaborative relations and little initial motivation to work together to benefit the community. The group included no commercial insurance or Medicare stakeholders, who might have driven a conversation about the need to control cancer care costs. Over a two-year period, the group was unable to develop a shared vision. Then one hospital revealed that it had secretly been developing plans for a new cancer center. The revelation destroyed what little trust existed among the partners, and the group broke apart.
The Dixie Solo County Collaborative also serves as a cautionary tale. Its membership composition was impressive: several major hospitals and health-care centers, a wide range of social service organizations, members of the local business community, health plans, and representatives of the faith community who together reflected broad-based leadership. This group was eager to work together to promote better community-wide population health as part of a larger effort to make the region attractive to businesses and their employees. Unlike the previous example, this group’s leaders were not focused solely on advancing their own institutions; they also embraced a common vision for community change.
However, the group failed to define a shared vision for the problems it should address and did not initially have a backbone infrastructure to support project work. Participants contributed little funding themselves and instead sought to secure outside funding as a first major step. But instead of working together to create a single funding proposal, they submitted three proposals that they were confident would get funded. None was successful, and they lost momentum.
Members of the group then undertook scattershot projects with little shared focus. The collaborative was later relaunched, after a different organization agreed to take it on. However, once reconstituted, it continued its fragmented approach to pursuing independent topics. One of its three individual work groups developed a focused strategy, secured funding, and made progress, but the other two work groups failed to make much headway. After two years, many stakeholders stopped attending meetings, and only the hospitals remained. The broad vision that the initiative set out to achieve narrowed to a hospital-centric focus on delivering care.
These failed starts betrayed a lack of trust and poorly articulated shared visions and strategies. Relationships that have a history of suspicion and mistrust spell failure. To manage these dynamics proactively, organizers can identify the stakeholders who are involved, or should be involved, in the issue and conduct interviews with them before trying to convene the group. This step will surface tensions that may exist among potential members and enable organizers to consider whether and how to address them before proposing collaborative action.
These cases also demonstrated the time-sensitive nature of forming a shared vision and strategy. In the initial stages of an initiative, organizers must succeed in establishing in participants’ minds a collective understanding of the problem and an agreement that working together will be more effective in addressing the problem than acting alone. Organizers can help prepare participants for this step by guiding them through a collective process of gathering and analyzing information about the community’s problems. When participants have a shared grasp on the current situation and its risks and downsides, as well as its opportunities, they will be better prepared to strategize together.
A second possible trajectory is growth followed by stumbling and failure. This trajectory may be explained by a combination of reinforcing mechanisms that produce some growth in collaboration, as well as impediments. Six collaboratives had periods of growth followed by stumbles. Faltering collaborative capacity can lead to failure and dissolution if reinforcing mechanisms activate and accelerate the decline.
The West Coast Regional Collaborative was initially successful at convening stakeholders and building a backbone organization. The group was well positioned and diverse, and included leaders from local hospitals and clinics, county-based public- and mental-health systems of care, policy makers, the business community, and patient advocates. These leaders had a strong inclination to work together to improve health-care access and coverage while also addressing health and wellness. People saw themselves as leading on behalf of the community and invested time and money in the work. They construed positive outcomes for the community as positive outcomes for themselves.
The group secured a large grant to work on improving access to care through a shared insurance-coverage program, but then stumbled when state funding for its health-care access program was cut. All other projects were tied to this funding stream, and the collaborative’s entire agenda faltered. The major hospital took over running the new health-care access program that the group had built and thereby provoked mistrust, because some stakeholders believed the hospital was motivated by self-interest. The group tried to reestablish itself based on two new initiatives: Medicaid reform and a health information exchange. When it failed to achieve either initiative, the group went dormant. Some of its members later rallied around a different group, led by stakeholders who had been left out of the first group.
Similarly, in another case, a hospital’s CEO received a $150,000 grant to provide care to the underserved and formed the Mid-Atlantic Health Alliance. He convened leaders from an array of providers in the region, and they launched new preventive-care programs. But the alliance stalled when the initial funding ran out, and the board became deadlocked over how to underwrite the effort. The member hospitals would not contribute funds because they viewed the new care programs as a potential competitor. Unfortunately, the alliance did not collect data or communicate effectively to the hospitals about how its programming might help save them money by preventing costly emergency room visits—an effort that could have reestablished trust and motivated further collaboration.
A short-lived recovery came when various medical-service providers and other local groups, such as career-services and disability-services providers, coalesced to provide a safety net for whatever people needed, such as access to care for the uninsured and dental care for people who could not afford to pay. The collaborative worked with the local hospitals but did not receive funding from them. Instead, it translated community needs into independent tasks that it could cover by applying for a patchwork of small grants from state, county, and local philanthropic sources. The presence of new collaborative activities, sources of funding, and health impacts endeared participants to the partnership, motivated them to collaborate, and encouraged stakeholders to invest resources. A long period of growth ensued but, unfortunately, ended in a major stumble. A failure to develop sustainable funding flows independent of short-term grants caused the collaborative to struggle constantly with money and curtail the access it had been able to provide.
Such cases illustrate what can happen when leaders don’t continually optimize a collaborative’s ability to agree on a shared vision, fail to formulate objectives against which progress can be measured, and lack the resources needed to sustain ongoing efforts. An initial strong start can falter if the collaborative commits to undertaking a subsequent set of tasks that exceed the management capability of the collaborative infrastructure, or if the collaborative does not develop sustainable sources of funding and runs short on money. The loss of momentum then initiates a downward spiral that results in greatly reduced motivation for continued collaboration. Collaborative leaders must stay vigilant in attending to the dynamic interplay of these factors over time. Many collaboratives begin with an initial seed grant but then get caught up in doing the work and don’t budget enough time for long-term planning. A regular review of the purpose of the collaborative—its reason for existing—can help leaders align strategic priorities, funding, and capacity.
A third kind of trajectory involves early stumbles followed by recovery. The Midwest Health Information Exchange Collaborative (the Exchange) experienced initial success with a narrow focus on health-care access for the underserved. Attracted to the collaborative by a widely admired community leader, members of the initial partnership applied for a state planning grant and used it to develop a broad health improvement strategy for the region. The magnitude of the Exchange’s vision and the presence of a state grant attracted additional partners from the community and public-health leaders, and that support reinforced the motivation to collaborate. However, the Exchange unexpectedly declined when it sought resources to launch more initiatives and broadened its focus beyond providing care for the underserved in order to apply for a massive grant with a short deadline. When it failed to secure the grant, the lack of funding meant that continuing an ambitious array of efforts rapidly exceeded the capacity of the Exchange’s existing infrastructure.
The collaborative eventually recovered by paring down its commitments to a handful of joint projects that could be undertaken with limited resources and a focused backbone organization. The Exchange also served as a convener, connecting other health leaders in the community and getting them to undertake additional projects independently of the Exchange’s core funding. The success of these initiatives in expanding care access and improving health outcomes increased its credibility and enabled the Exchange to apply for other sources of funding and expand its infrastructure to support further work under its own management.
If stakeholders are enthusiastic about initiatives that diverge from the collaborative’s main focus, helping them find additional resources is preferable to diluting those of the collaborative.
The collaboratives that stumbled, then recovered, demonstrate the importance of a good match between infrastructure (e.g., a backbone organization) and the scope of the activities the collaborative undertakes. Pursuing an ambitious set of projects might seem attractive for promoting growth but can also impede growth if the infrastructure cannot provide the necessary levels of coordination and support. An unfocused, expansive vision of what the collaborative can achieve can generate an overly ambitious set of projects. Spreading resources among too many different initiatives can leave all of them with too little support to have an impact.
To reverse early stumbles of the sort that the Exchange experienced, or to avoid them altogether, a more selective strategic focus based on high-leverage initiatives that reinforce interdependencies among stakeholders can help. If stakeholders are enthusiastic about initiatives that diverge from the collaborative’s main focus, helping them find additional resources is preferable to diluting those of the collaborative.
The fourth trajectory, which we observed in seven collaboratives, is sustained growth of capacity. We learned that this trajectory typically results from a delicate balance of strategies that take full advantage of reinforcing mechanisms to promote the growth of collaboration while avoiding or minimizing impediments and unintended consequences.
Some collaboratives with sustained growth trajectories started with small projects all or most participants could agree on and moved to more controversial issues, such as addressing competition between hospitals, only after first establishing trust, accomplishing real impact, learning from experience, and establishing value in the community. Some of the collaboratives attracted additional resources, including funding, new members, and new personnel, by measuring and communicating the beneficial health and health-care impacts they achieved. Growth of this sort was not uniform; rather, it often resembled a stairstep pattern or even a series of small stumbles and recoveries that moved steadily upward over time.
The longest-standing collaborative in our sample, Rocky Mountain Health, started with a broad, diverse base of stakeholders. Partner organizations agreed to participate in an internal tax system within a local health plan. That tax system provided sustainable financing for infrastructure support and operational management of early care initiatives. The founders launched a nonprofit organization to receive the funds, hired staff to lead health initiatives, and collected and provided data about health and health-care costs and savings.
In addition, the new entity was able to pay funds back into the provider network and therefore created a positive cycle of motivation for members to support the collaborative. The infrastructure also made it possible for members to launch an increasingly wide array of health initiatives, many of which helped reduce the costs of care while expanding access. This virtuous cycle eventually led the collaborative not only to produce excellent health outcomes but also to maintain some of the lowest per capita health-care costs in the nation. Leaders of this initiative credited their success to an intentional practice of reflecting on what they achieved, what contributed to that achievement, and what got in the way, then re-adjusting shared goals to ensure that all partners were committed to the collaborative’s success.
These success stories demonstrate the importance of using initial impact to enhance a collaborative’s capacity for additional impact. This strategy starts with measuring and communicating impacts to stakeholders and the broader community, including potential funders and new participants. The collaborative and its backbone organization should also find a way to benefit from additional resources. They can do so by dedicating portions of grants that specifically support the backbone organization. Alternatively, resources can come from an internal tax system in which certain stakeholders provide sustainable funding. These funds could, for example, accrue from increased revenues or decreased costs that result from the collaborative’s impacts (e.g., savings from preventive-health programs). Shared savings arrangements are becoming increasingly prevalent in programs such as accountable care organizations (ACOs). ACOs encompass groups of health-care providers in a region. They operate with a fixed overall budget, and greater efficiency can produce savings, some of which those providers and the ACO retain.
Strategies for Growing Collaborative Capacity
As we have seen, our research into the dynamic framework and how it shaped collaboratives’ different trajectories surfaced important lessons that can inform leaders. To generalize, we found four specific strategies for developing and sustaining successful collaboratives.
First, a collaborative must start by creating the necessary conditions for success. It must begin by convening the actors that represent the different facets of the major health problems facing the region it serves and the capabilities necessary for dealing with them. Once these stakeholders are assembled, they need to create governance structures that assure that all participants’ voices will be heard and interests respected. Apportioning decision rights equitably will build trust, as will adopting goals, priorities, and metrics that members establish mutually. Members must also articulate a shared purpose for the entire group, and goals to be pursued collectively if the shared purpose is to be achieved. Member organizations then need to identify opportunities to align their priorities and incentives, including organizational reward structures, with these goals.
Second, a new collaborative needs to choose its early projects strategically. It should begin by creating a convergent process for selecting initial priorities and projects. The process must initiate action swiftly, or members will lose motivation and interest. The collaborative should choose projects that require multiple organizations and cannot be done alone by any of them, that further the purpose of the collaborative and member organizations, that can show measurable progress and benefit within a reasonable amount of time, and that can be accomplished with minimal resources. By the time projects are selected, the collaborative should also have tracking systems in place to measure progress and ensure that early projects are meeting their objectives. The collaborative should also publicize early wins to members and the community at large to motivate continuing support.
As early projects produce perceived benefit and motivate members to become more deeply involved, members of the collaborative should next make a series of investments that help expand capacity and set the stage for more ambitious initiatives. These investments should provide a foundation for the collaborative’s sustained impact. The collaborative needs to start by building an infrastructure (backbone organization) that can coordinate members’ efforts and various projects. The backbone organization should perform or assign important staff functions, such as pursuing funding and publicizing the collaborative’s accomplishments. Staff and other resources may be borrowed from member organizations, but the backbone organization must clarify who is responsible for the work.
A functional collaborative must continuously review how the collaborative itself is functioning. Are members remaining actively involved? Are they supporting the collaborative’s goals?
One critical function of this staff is helping to create a diverse set of funders that allow the collaborative to avoid overdependence on any single source of support. Successful efforts that attract funding from outside sources can further motivate members to remain involved and make their own investments in the collaborative and its initiatives.
The backbone organization should also develop systems for research and data analysis. These systems can, for example, highlight complex community problems that affect multiple participants and cannot be solved by any single organization or sector, thereby helping the collaborative to select high-priority projects. Backbone organization staff can then identify initiatives for dealing with those problems, drawing on evidence-based strategies and best practices used by other communities. Once staff have selected these initiatives, the systems can track their progress, help them to remain well coordinated and on schedule, and enable the collaborative to communicate the resulting community benefit.
Fourth, the collaborative should initiate a self-monitoring process at the beginning and revisit it throughout its entire life span to ensure that it is adequately supported. A functional collaborative must continuously review how the collaborative itself is functioning. Are members remaining actively involved? Are they supporting the collaborative’s goals or protecting their own organizations’ interests? Are the infrastructure and processes adequate for undertaking the desired set of initiatives? Do members understand the perspectives of systems leadership—do they see the impacts of the collaborative as catalysts for change within the larger set of forces affecting a region’s health? Are there processes in place that build on successes to grow collaborative capacity? Answering these questions needs to be part of a learning process that builds the ability to collaborate effectively based on thoughtful reflection about experience with collaborative tasks. This “learning loop” is an essential component of the larger growth loops driving collaborative capacity.
Pitfalls That Reduce Collaborative Capacity
Our research also indicated a number of ways in which collaboratives can get into trouble and potentially fail. One impediment that can bedevil collaboratives at an early stage is the inability to focus on and select initiatives to undertake. This failure can result from an overly broad vision or lack of a clear vision. The inability to focus can lead to dialogue fatigue, reduced motivation, and member organization dropout. Too narrow a vision, on the other hand, can limit the scope of collaboration and the impact it can produce.
Choosing a focus is subject to a number of trade-offs that complicate the process. Including a broader, more diverse set of members can expand the range of problems and solutions but, conversely, can make focusing on a manageable set of tasks harder. At the early stages, collaboratives may want to adopt initiatives that represent a balance between satisfying participants’ diverse interests and avoiding the risks of an inability to focus. This means projects must represent a scope that is achievable, even if at first they seem more limited in importance and community benefit than stakeholders might desire.
Collaboratives can manage their initiatives in ways that also create problems. They can take on too many (or too broad) tasks beyond what the collaborative infrastructure can support, thereby reducing impact and undermining perceived accomplishment. They can also take on tasks that require a higher degree of interdependence among organizations than the collaborative infrastructure can handle, causing poor coordination and reduced impact. Collaboratives may be overly optimistic and set expectations too high for task accomplishment. When expectations are not met, low perceived benefit and reduced motivation for further collaboration result.
Furthermore, several of the collaboratives we studied stumbled because of their failure to develop diverse, sustainable funding flows. In some cases, the collaborative relied on a single large grant that didn’t materialize or ended with the collaborative’s needing more support. By constraining resources available for programs and infrastructure development, this shortfall reduced the collaboratives’ ability to achieve measurable impact on the community’s health or benefits for participants.
Dynamic Leadership
The final essential lesson from our work is the importance of dynamic thinking by leaders. Our model suggests a leadership approach informed by a systemic, dynamic view that collaborative capacity is a function of multiple factors that influence one another in nested feedback loops. Leadership that changes one feature creates consequences—both intended and sometimes unintended—on other parts of the system, and those in turn affect the initial feature.6
Dynamic thinking is a different way of leading than one that follows linear checklists of suggested actions. For example, checklist-style thinking may draw one’s attention to the need to find funding to launch a project. Dynamic thinking, by contrast, asks leaders to finance a project that will generate the capacity to attract future funding for the collaborative as the success of the project produces or attracts additional investment. Shared measurement systems are important; the dynamic perspective illustrates why they are important. They can provide evidence of both need and impact and thereby increase participating organizations’ motivation. Financing mechanisms, such as shared savings arrangements, can also help turn measurable impact into additional resources for more capable infrastructure and other impactful projects. Similarly, all collaboratives need to define a clear purpose—a point that nearly all the checklists in the literature emphasize. But dynamic leadership requires that purpose to be translated into a set of projects that help to achieve the purpose while being appropriately matched to the collaborative’s infrastructure and capacity to undertake those projects. However, undertaking a good set of projects is not enough. They must be done in the right sequence in order to sustain a positive trajectory for the collaborative.
Dynamic thinking favors launching multiple, interrelated actions together, rather than attacking one item on a checklist at a time, because such a strategy can generate positive feedback effects that can increase capacity and strengthen the collaborative. This mindset encourages leaders of backbone organizations to bundle sets of actions into manageable chunks; set aside time to consider the intended and unintended consequences of the proposed plan of action; sequence growth to set a positive flywheel in motion; and allow sufficient time for reflection, learning, and adjustment at regular intervals. By building on mutually reinforcing actions and avoiding unintended consequences, leaders can help to assure that a collaborative sustains itself, grows, and succeeds in achieving its intended purposes.
Want to hear more from the authors of this article? Listen to their interview on Spring Impact's Mission to Scale podcast, part of a special series with the authors of SSIR's Summer 2022 issue.
Read more stories by Gary Hirsch, Kate Isaacs & Ruth Wageman.