

Imagine a medicine that could keep you healthy for the rest of your life. Would you take it? Of course. Now imagine that you have to remember to take this medicine every day, and endure unpleasant and sometimes incapacitating side effects. Would you still take it as prescribed? Maybe, maybe not. What if you had to travel out of your way and lose wages to pick up the medicine—all while trying to conceal your condition so that you could avoid the stigma associated with disease? Would you still take it?
Unfortunately, many people do not take their medicines as prescribed—an issue that the medical community has come to call “poor medication adherence.” This is a widespread and dangerous problem. A recent trial that provided antiretroviral drugs to women in sub-Saharan Africa to prevent HIV, for example, failed to prevent new infections because participants did not regularly use the product. Treatments are naturally less effective when patients take them inconsistently, and poor adherence can lead to bigger and costlier health challenges such as drug resistance and higher disease transmission rates.
We explored the issue of medication adherence in the context of HIV treatment in Tanzania, where a startling 5 percent of the population is infected with HIV. Our research team, which includes top-notch epidemiologists and health economists, knew a lot about the academic literature, but we realized there was a big gap in understanding our population of interest. What was the patient experience? What happens in the clinic that dissuades patients from heeding staff’s advice? What happens at home to prevent patients from following a particular course of care? Traditional public health research alone couldn’t help us answer these questions, so we decided to tackle adherence from a different vantage point—to follow the lead of those who are applying human-centered design to social challenges and who advocate for a customer-centered approach to global health.
We ventured into this uncharted territory with support from the Grand Challenges Exploration Program of The Bill & Melinda Gates Foundation. We set our sights on Shinyanga, a city in northern Tanzania, and articulated four guiding steps—watch, listen, map, and test —in the hopes that they would frame our work in a useful way, and help us come up with a simple way to promote adherence .
Watching
With the help of local research assistants we used disciplined observation to watch the patient flow through HIV clinics, adherence counseling sessions, and patients’ routines at home. We counted how many patients actually looked at posters outlining the benefits of adherence. We counted how many positive or negative comments staff made to patients about patients’ adherence practices. And we tracked how often patients sought advice from one another. Our findings suggest that patients will travel miles out of their way to avoid visiting an HIV clinic close to their homes where they might be recognized, but when they arrive at the clinic they recognize many other patients who share their appointment days, and they don’t mind being recognized by these individuals. In this way, the waiting room is an informal source of social support.
Listening
We asked a lot of questions and listened closely to the answers. Patients told us what adherence actually implied for their day-to-day life, but they also shared their individual reasons for staying healthy, and who and what they wanted to live for. Taking the time to listen to patients helped us understand exactly why a system of care that treats all patients the same doesn’t help with adherence. A young healthy woman who comes in for another service and unexpectedly receives a HIV positive diagnosis is fundamentally different than an older patient with more debilitating symptoms who may have suspected his or her diagnosis for weeks. These patients have vastly different experiences with and attitudes about treatment.
Mapping and Brainstorming
Using the insights from our qualitative work, we grouped patients into five distinct segments and then created “customer journey maps” to chart the experiences of each of these segments from diagnosis to long-term adherence behavior.
See larger version. (Image by Kate Sallai)">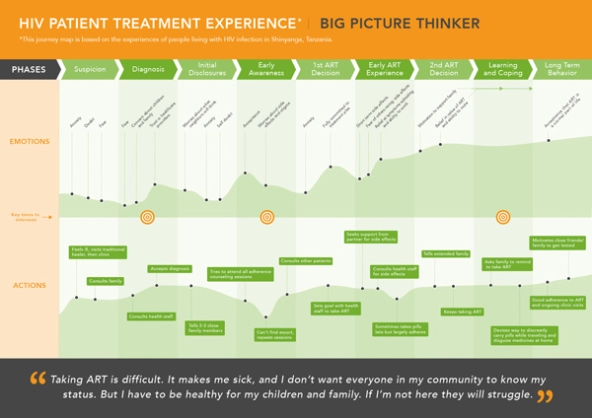 This map represents important stages in the Big Picture Thinker’s experience with HIV treatment that influence adherence behavior. See larger version. (Image by Kate Sallai)
This map represents important stages in the Big Picture Thinker’s experience with HIV treatment that influence adherence behavior. See larger version. (Image by Kate Sallai)
We also created short personas to represent each segment. These profiles offer the patient’s perception of what health means to them, what might keep them from taking their medications regularly, and what types of interventions would help them follow their treatment plan consistently. Businesses commonly use these types of customer journey maps and personas to guide business model and marketing innovation, but we had never come across these tools in a global health context.
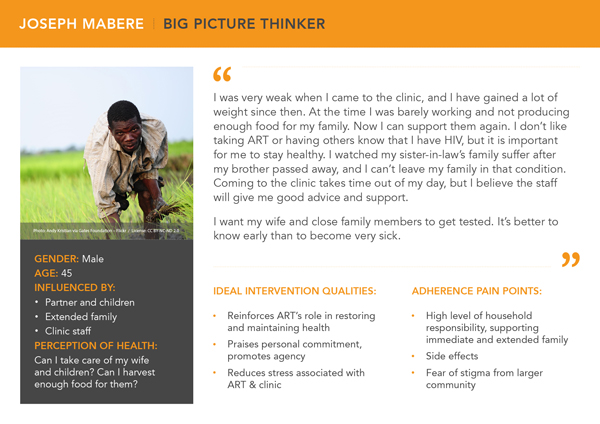 This fictional persona represents a typical patient that belongs to the Big Picture Thinker segment. Personal responsibilities such as caring for their children motivate these patients to adhere, despite the obstacles they face. (Image by Kate Sallai)
This fictional persona represents a typical patient that belongs to the Big Picture Thinker segment. Personal responsibilities such as caring for their children motivate these patients to adhere, despite the obstacles they face. (Image by Kate Sallai)
These tools helped us hone in on the most important barriers to adherence. For instance, we learned that patients go to great lengths to hide their need for treatment from others due to the stigma of HIV/AIDS. We also found that the average patient has strong aspirations for the near future, such as returning to farm work or getting married, and these goals, which can motivate health behaviors, rarely come up in conversations with care providers.
These tools also helped us brainstorm solutions. Once we narrowed down our list of ideas, we tested them with patients using early prototypes. We’ve continually iterated on these ideas, and our current frontrunners include a pillbox with the rough dimensions of a feature phone that allows patients to carry pills more discreetly, materials that relate adherence to patients’ immediate social goals, and priming (or “nudge”) tactics that remind patients of the social support available to them at the clinic. By testing and rapidly incorporating feedback, we have been able to design materials that resonate with patients. Over the next few months, we will offer these materials in select clinics and test the effects using traditional epidemiological methods. If they’re successful, we’ll work with the Ministry of Health and Social Welfare in Tanzania to refine our interventions, and provide them to more facilities. If they fail, then at least we have a strong foundation on which to try again.
Behavior change isn’t just about crafting the perfect message; creating better programs requires really listening to and understanding the patient experience. We believe that taking a patient-centered approach and borrowing tools from the private sector that were developed to understand, track, and influence customers can greatly enhance global health programs that require changes in attitudes or behavior. Adherence is just the beginning.
Read more stories by Aarthi Rao & Sandra McCoy.