

 (Illustration by iStock/ma_rish)
(Illustration by iStock/ma_rish)
“Every system is perfectly designed to get the results it gets,” physician and health-policy expert Paul Batalden said.1 This much-repeated quote captures a way to conceptualize equitable implementation that takes into account factors like the history of racial discrimination and access to health care when studying why disparities exist and assessing the needs of a community to eliminate them.
Bringing Equity to Implementation

Implementation science—the study of the uptake, scale, and sustainability of social programs—has failed to advance strategies to address equity. This collection of articles reviews case studies and articulates lessons for incorporating the knowledge and leadership of marginalized communities into the policies and practices intended to serve them. Sponsored by the Anne E. Casey Foundation
-
Equity Is Fundamental to Implementation Science
-
Trust the People
-
Youth Leadership in Action
-
Community Takes the Wheel
-
Equity in Implementation Science Is Long Overdue
-
Listening to Black Parents
-
Faith-Based Organizations as Leaders of Implementation
-
Community-Defined Evidence as a Framework for Equitable Implementation
-
Community-Driven Health Solutions on Chicago’s South Side
-
Equitable Implementation at Work
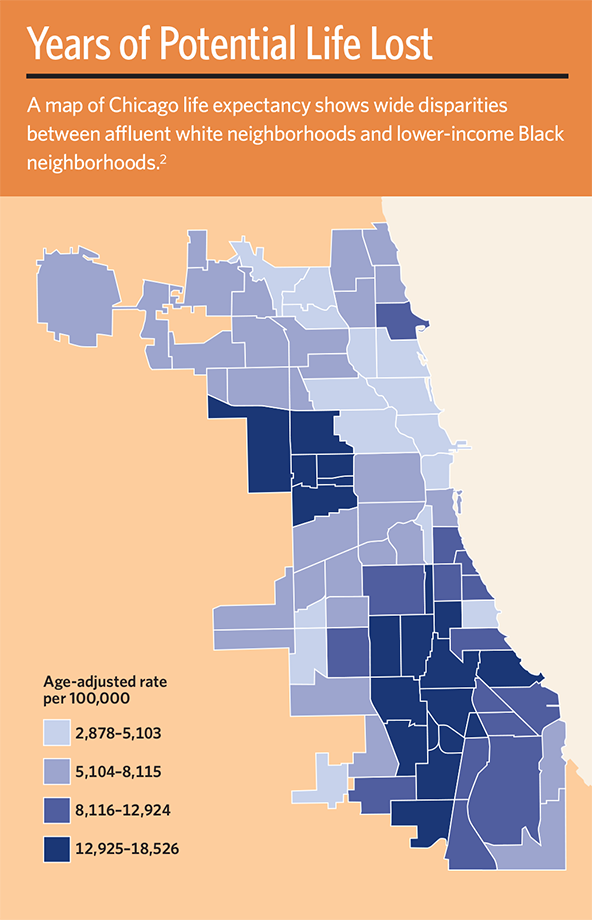
Some very alarming statistics reveal population-level disparities within our social and health-care systems. One prominent example is the 30-year gap in life expectancy between people living in the poor, predominantly African American neighborhoods on Chicago’s South Side, as compared to those in the more affluent, predominantly white neighborhoods just nine miles away in Chicago’s Loop. This is the largest life expectancy gap in the United States, according to the City Health Dashboard,2 and is attributable to few economic opportunities and high rates of obesity, diabetes, hypertension, heart disease, and stroke in South Side neighborhoods.3 The origins and ramifications of this wide difference in life expectancy are deeply, systemically entrenched and must be acknowledged if we are to effectively close the gap.
Although the COVID-19 pandemic has underscored the urgent need to tilt health-care systems toward equitable outcomes,4 the causes are rooted in centuries of systemic racism, economic exploitation, and other factors. Further, mistrust of the health-care system and of medical research runs deep in communities of color,5 and for good reason. For example, in the Tuskegee Study, which ran from 1932 to 1972, the US Public Health Service and the Centers for Disease Control and Prevention intentionally withheld treatment from African American men with syphilis in order to study the progression of the disease.
A primary way to advance health equity is to focus exclusively on implementing interventions in communities that experience disparities in treatment. Simply including populations with disparities in larger studies with nondisparity groups potentially neglects the need for strategies that address underlying structural causes of the disparities, such as the disinvestment in communities of color that has resulted in scarce and under-resourced health-care systems.6
You need both fertile soil and viable seeds for plants to thrive, yet medical research too often focuses on the seeds while neglecting to cultivate the soil. The field of implementation science aims to improve health outcomes by studying how to deliver the best available interventions (i.e., the seeds) in a manner that overcomes barriers and leverages individual, system, and community assets (i.e., the soil).7 Using implementation science to address health inequities has only recently become an explicit goal—even though a prominent report by the National Academy of Medicine declared equity, which they define as quality care that does not vary simply because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status, as a standard back in 2006.8
To establish equitable health care, customized awareness, and accessibility and availability of interventions, implementation researchers must bring the voices of community members to the forefront and integrate those voices throughout their work. How researchers engage with the community is critical for the sustained success of any improvement initiative. The key to hearing and listening to the community starts with creating synergy among trusted voices on a particular health-related goal.
Below we detail the key ingredients to achieving equitable implementation of an intervention for hypertension among African American adults living in Chicago. Our three-pronged strategy includes understanding the specific challenges identified by the community that need immediate attention; intentional inclusion of community stakeholders as early as possible in order to prioritize their perspectives; and building and delivering tangible resources for addressing the needs expressed by the community. Doing so will yield enduring solutions and effective strategies required to address awareness of, access to, and capacity for implementation of better interventions in these communities.
Partnering With the Community
Implementation science has long recognized the critical role of meaningful partnerships with the various persons and entities that are involved in the delivery of new interventions,9 but it is often underdeveloped and not explicitly leveraged in service of achieving equity. Much of the focus has been on the partnership between academic researchers and more traditional health-care delivery systems, such as safety-net community health centers (CHCs).
Years ago, the three of us began setting the groundwork for a seven-year project focused on hypertension among African American adults, with equitable implementation at the fore. We officially began the project, called Community Intervention to Reduce CardiovascuLar Disease in Chicago (CIRCL-Chicago), in August 2020. In CIRCL-Chicago, our partnership model included working with Pastors for Patient-Centered Outcomes Research (P4P), which is a hub for faith-based communities and leaders interested in research engagement.10
Since its inception in 2013, P4P has successfully engaged church congregations and leaders in health-related initiatives.11 Even for nonreligious individuals, churches in predominantly African American neighborhoods serve as crucial anchors and trusted voices for community gathering, resources, and support.12 P4P includes stakeholder input by actively listening, proactively involving, and quickly training members of the community—not as segregated contributors but as members of a collaborative partnership. CIRCL-Chicago takes this partnership model a step further by connecting churches with CHCs in the same neighborhoods to both engage participants in the process and to deliver the intervention. Our approach includes the voices of people who have experience both with hypertension and with the local health-care system.
Community-Driven Interventions
P4P leads community-driven processes for identifying health priorities to give local churches a voice in how to care for community members. In 2016 and 2018, P4P administered a 10-item community health assessment to 836 residents living in 12 ZIP codes that corresponded to member churches.13 High blood pressure was the highest-rated health priority both years. This priority is consistent with the high prevalence of hypertension among African Americans both in Chicago and across the United States.14
In planning CIRCL-Chicago, we convened diverse stakeholders, including P4P leaders, academic researchers, community-based research organizations, CHCs serving our study community, and representatives from organizations such as the American Heart Association and American Medical Association. We jointly selected an evidence-based, multicomponent intervention for high blood pressure comprised of evidence-based blood pressure-control guidelines, a health system-wide hypertension registry, quarterly blood pressure-control reports, follow-up visits for blood pressure measurement and management by health-care professionals, and promotion of single-pill combination pharmacotherapy.15
Developed and tested by the Kaiser Permanente of Northern California’s health-care system, this multicomponent intervention is now being adapted to the context of Chicago’s South Side neighborhoods in partnership with community members. Prior efforts to translate the Kaiser intervention bundle to CHCs were successful, but less so than the trial by Kaiser Permanente of Northern California that first established its effectiveness.16 This suggests there is a need for a focused effort to implement the bundle in a way that is both acceptable to community members and feasible to implement.
Plotting the Course Ahead
Now six months into the project, CIRCL-Chicago has met with leaders from churches, local CHCs, P4P and members of the community who might participate in the intervention, local and national professional organizations, and academic experts in implementation science, blood pressure control, informatics, and community-engaged research. Based on these meetings, we are following an established process for adapting the intervention17 to ensure a systematic and comprehensive approach that stays true to the core aspects of the Kaiser bundle responsible for its effectiveness, while making necessary adaptations for the intervention to be successful in the local community.
For example, P4P ensures that the initial program messaging is delivered from a trusted community voice and makes certain that in every face-to-face meeting, familiar faces are there to provide service and answer questions. We plan to enlist such community health workers to take blood pressure measurements instead of using medical assistants. We hope this strategy will help mitigate mistrust of the health-care system that patients may experience and reduces the burden on understaffed CHCs.
We also propose a registry that will provide blood pressure-control reports. The goal of this platform is to enable the sharing of data concerning participants’ blood pressure and treatment across care settings such as churches and CHCs to create enhanced opportunities to identify and treat people with hypertension. P4P’s practices include free-of-charge follow-up contacts to ensure honest and consistent communication, including virtual meetings to discuss progress and findings.
The CIRCL-Chicago project will first see whether the adapted Kaiser intervention bundle can be delivered in a small number of churches and CHCs. Early testing of the implementation provides critical data to inform the ongoing process of adaptation that is constantly informed by the community. Next, we will begin a community-level trial within the South Side Chicago neighborhoods that experience the greatest disparities in hypertension and cardiovascular health outcomes.18 Within these neighborhoods are approximately 16 churches that are part of the P4P network and 12 CHCs that are members of two health-center networks, AllianceChicago and Access Community Health Network.
Based on estimates of the prevalence of uncontrolled blood pressure in these neighborhoods, we expect to enroll between 600 and 1,800 participants in the adapted Kaiser intervention bundle, and we will compare our outcomes to participants residing on Chicago’s West Side—an area with similar disparities in hypertension rates to the South Side—that are receiving the usual health care in their community.
CIRCL-Chicago seeks to comprehensively evaluate the implementation of the Kaiser intervention bundle.19 To determine whether the implementation is successful, we will track the proportion of eligible adults in the community that experience blood pressure control (i.e., <130/80 mm Hg) from the intervention. We will also dig deeply into these data to understand the representativeness of the participants that are referred to and receive the Kaiser intervention bundle, and those that experience blood pressure control.20 CIRCL-Chicago will be implemented in neighborhoods that are predominantly African American, and we will focus on patient age, gender, insurance status, and health-care system variables that could lead to inequity within this population. Any differences that emerge signal the need for deeper exploration to understand the nature and cause of variable impact.
CIRCL-Chicago’s community-driven approach shows that neighborhoods like the South Side, and indeed many other communities across the United States, need investment in different implementation strategies and resources than those used to support implementation in other populations. Neglecting this reality has the potential to exacerbate disparities through inequitable implementation.
The premium often placed on generalizable findings in implementation research runs the risk of assuming equality is the answer. But real solutions are only possible with equitable strategies that recognize the contribution of historical and contemporary policies, economics, and health-care access, among other factors—the consequences of which are repeatedly underscored in health disparities. Community-driven, equitable implementation approaches hold the key to unlocking sustainable solutions to eliminate health disparities that are embraced by the community. A key driver of sustaining this intervention hinges on fostering co-leadership, co-ownership, and equal decision-making among all partners and stakeholders.
Read more stories by Abel N. Kho, Justin D. Smith & Paris Davis.